

Dangers of hyperoxia
- PMID: 34924022
- PMCID: PMC8686263
- DOI: 10.1186/s13054-021-03815-y
Dangers of hyperoxia
Abstract
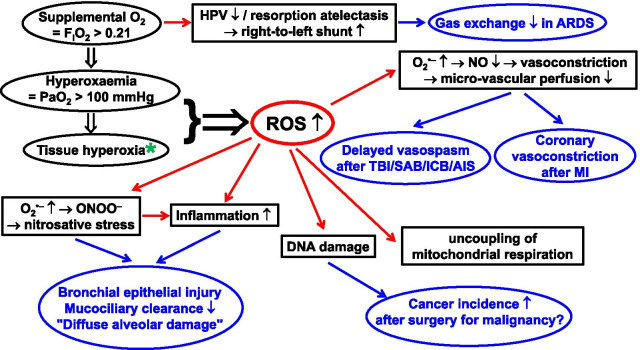
Oxygen (O2) toxicity remains a concern, particularly to the lung. This is mainly related to excessive production of reactive oxygen species (ROS). Supplemental O2, i.e. inspiratory O2 concentrations (FIO2) > 0.21 may cause hyperoxaemia (i.e. arterial (a) PO2 > 100 mmHg) and, subsequently, hyperoxia (increased tissue O2 concentration), thereby enhancing ROS formation. Here, we review the pathophysiology of O2 toxicity and the potential harms of supplemental O2 in various ICU conditions. The current evidence base suggests that PaO2 > 300 mmHg (40 kPa) should be avoided, but it remains uncertain whether there is an "optimal level" which may vary for given clinical conditions. Since even moderately supra-physiological PaO2 may be associated with deleterious side effects, it seems advisable at present to titrate O2 to maintain PaO2 within the normal range, avoiding both hypoxaemia and excess hyperoxaemia.
Keywords: ARDS; Acute ischaemic stroke; Cardiopulmonary resuscitation; Hyperoxaemia; Hyperoxia; Intracranial bleeding; Myocardial infarction; Reactive nitrogen species; Reactive oxygen species; Sepsis; Subarachnoidal bleeding; Surgical site infection; Trauma-and-haemorrhage; Traumatic brain injury.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests..
Figures
References
-
- West JB. Carl Wilhelm Scheele, the discoverer of oxygen, and a very productive chemist. Am J Physiol Lung Cell Mol Physiol. 2014;307(11):L811–L816. - PubMed
-
- West JB. Joseph Priestley, oxygen, and the enlightenment. Am J Physiol Lung Cell Mol Physiol. 2014;306(2):L111–L119. - PubMed
-
- West JB. The collaboration of Antoine and Marie-Anne Lavoisier and the first measurements of human oxygen consumption. Am J Physiol Lung Cell Mol Physiol. 2013;305(11):L775–L785. - PubMed
-
- Leverve XM. To cope with oxygen: a long and still tumultuous story for life. Crit Care Med. 2008;36(2):637–638. - PubMed
-
- Asfar P, Singer M, Radermacher P. Understanding the benefits and harms of oxygen therapy. Intensive Care Med. 2015;41(6):1118–1121. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
