

Intraoperative prediction of postanaesthesia care unit hypotension
- PMID: 34924175
- PMCID: PMC9074793
- DOI: 10.1016/j.bja.2021.10.052
Intraoperative prediction of postanaesthesia care unit hypotension
Abstract
Background: Postoperative hypotension is associated with adverse outcomes, but intraoperative prediction of postanaesthesia care unit (PACU) hypotension is not routine in anaesthesiology workflow. Although machine learning models may support clinician prediction of PACU hypotension, clinician acceptance of prediction models is poorly understood.
Methods: We developed a clinically informed gradient boosting machine learning model using preoperative and intraoperative data from 88 446 surgical patients from 2015 to 2019. Nine anaesthesiologists each made 192 predictions of PACU hypotension using a web-based visualisation tool with and without input from the machine learning model. Questionnaires and interviews were analysed using thematic content analysis for model acceptance by anaesthesiologists.
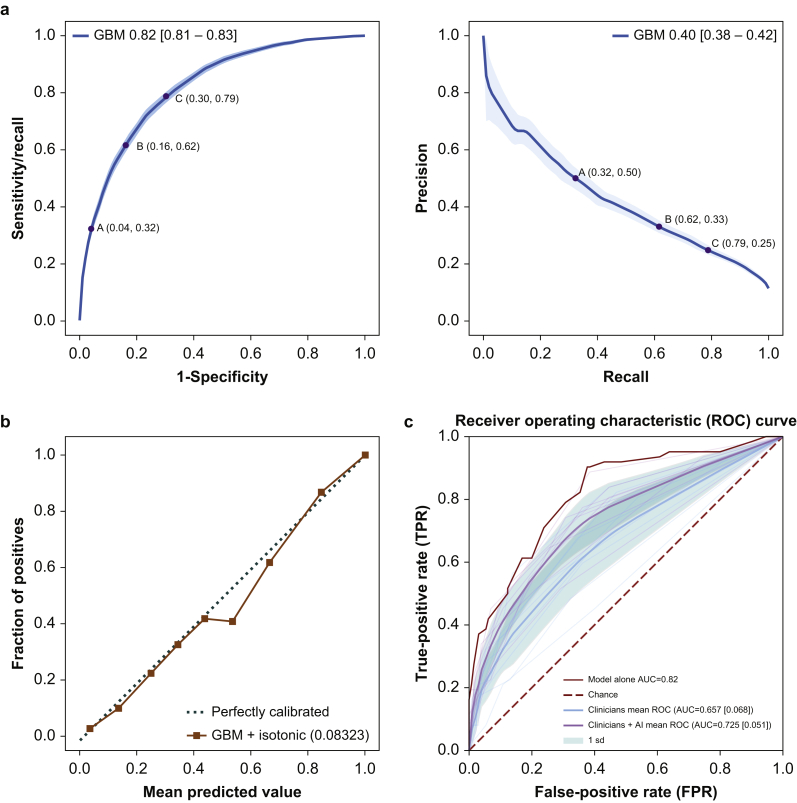
Results: The model predicted PACU hypotension in 17 029 patients (area under the receiver operating characteristic [AUROC] 0.82 [95% confidence interval {CI}: 0.81-0.83] and average precision 0.40 [95% CI: 0.38-0.42]). On a random representative subset of 192 cases, anaesthesiologist performance improved from AUROC 0.67 (95% CI: 0.60-0.73) to AUROC 0.74 (95% CI: 0.68-0.79) with model predictions and information on risk factors. Anaesthesiologists perceived more value and expressed trust in the prediction model for prospective planning, informing PACU handoffs, and drawing attention to unexpected cases of PACU hypotension, but they doubted the model when predictions and associated features were not aligned with clinical judgement. Anaesthesiologists expressed interest in patient-specific thresholds for defining and treating postoperative hypotension.
Conclusions: The ability of anaesthesiologists to predict PACU hypotension was improved by exposure to machine learning model predictions. Clinicians acknowledged value and trust in machine learning technology. Increasing familiarity with clinical use of model predictions is needed for effective integration into perioperative workflows.
Keywords: data science; hypotension; machine learning; postanaesthesia care unit; risk prediction.
Copyright © 2021 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures



References
-
- Salmasi V., Maheshwari K., Yang D., et al. Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: a retrospective cohort analysis. Anesthesiology. 2017;126:47–65. - PubMed
-
- Sessler D.I., Khanna A.K. Perioperative myocardial injury and the contribution of hypotension. Intensive Care Med. 2018;44:811–822. - PubMed
-
- Sun L.Y., Wijeysundera D.N., Tait G.A., Beattie W.S. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology. 2015;123:515–523. - PubMed
-
- Monk T.G., Bronsert M.R., Henderson W.G., et al. Association between intraoperative hypotension and hypertension and 30-day postoperative mortality in noncardiac surgery. Anesthesiology. 2015;123:307–319. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
