

Lung transplant recipients with idiopathic pulmonary fibrosis have impaired alloreactive immune responses
- PMID: 34924263
- PMCID: PMC9038662
- DOI: 10.1016/j.healun.2021.11.012
Lung transplant recipients with idiopathic pulmonary fibrosis have impaired alloreactive immune responses
Abstract
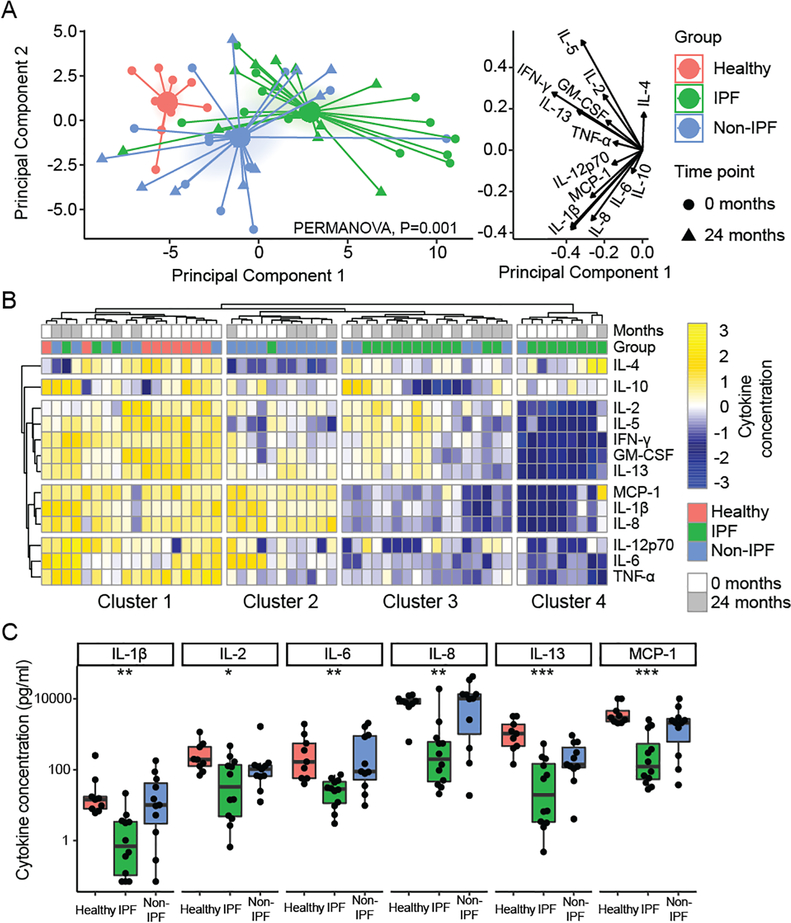
Background: Telomere dysfunction is associated with idiopathic pulmonary fibrosis (IPF) and worse outcomes following lung transplantation. Telomere dysfunction may impair immunity by upregulating p53 and arresting proliferation, but its influence on allograft-specific immune responses is unknown. We hypothesized that subjects undergoing lung transplantation for IPF would have impaired T cell proliferation to donor antigens.
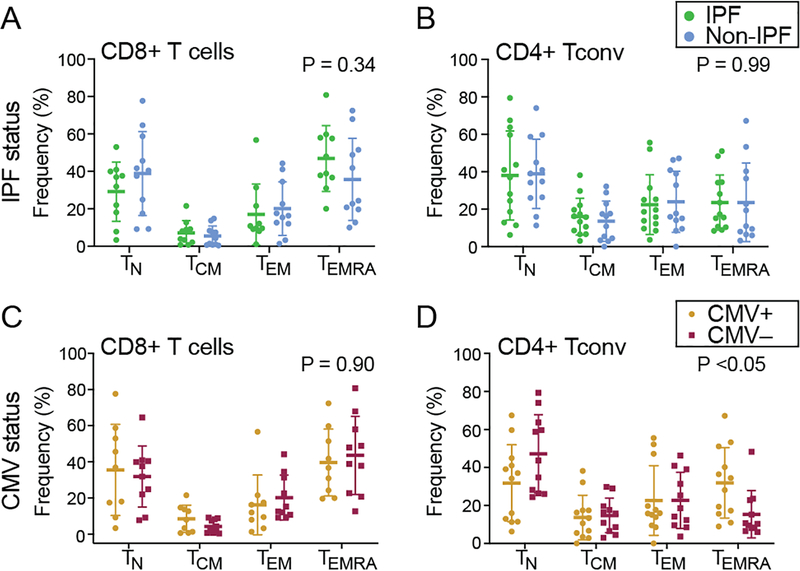
Methods: We analyzed peripheral blood mononuclear cells (PBMC) from 14 IPF lung transplant recipients and 12 age-matched non-IPF subjects, before and 2 years after transplantation, as well as PBMC from 9 non-transplant controls. We quantified T cell proliferation and cytokine secretion to donor antigens. Associations between PBMC telomere length, measured by quantitative PCR, and T cell proliferation to alloantigens were evaluated with generalized estimating equation models.
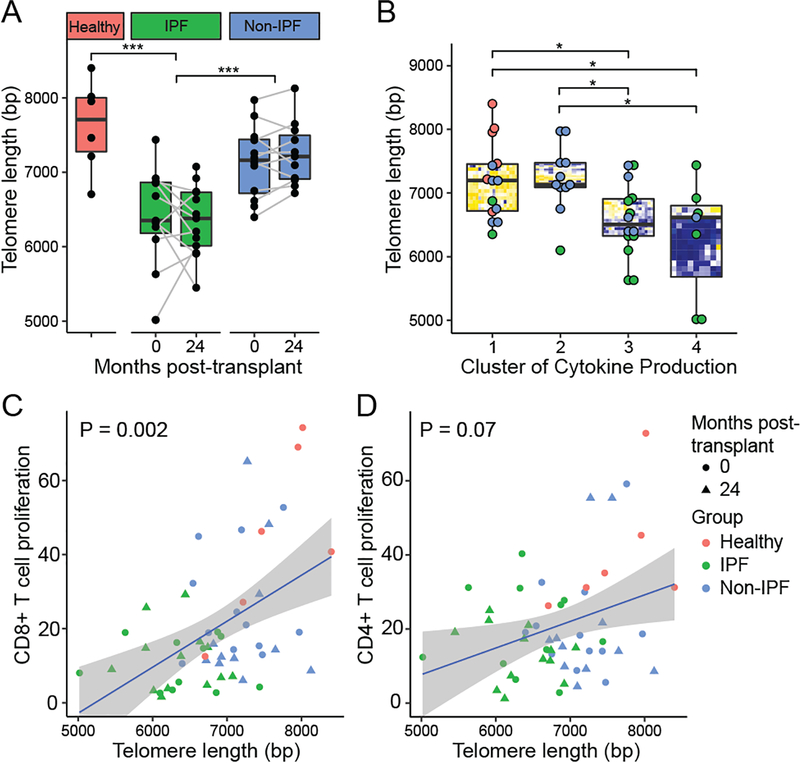
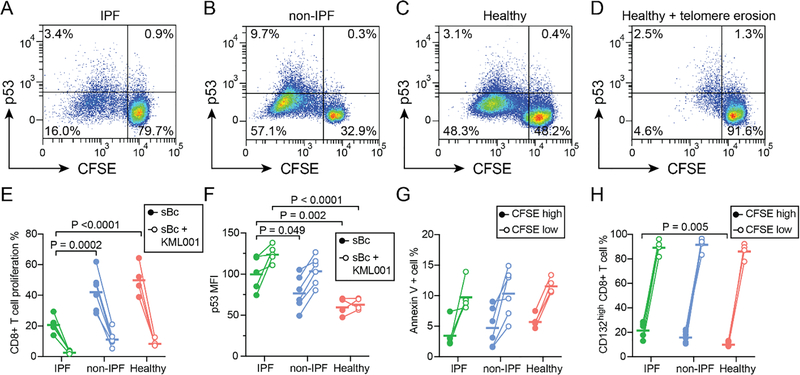
Results: IPF subjects demonstrated impaired CD8+ T cell proliferation to donor antigens pre-transplant (p < 0.05). IL-2, IL-7, and IL-15 cytokine stimulation restored T cell proliferation, while p53 upregulation blocked proliferation. IPF subjects had shorter PBMC telomere lengths than non-IPF subjects (p < 0.001), and short PBMC telomere length was associated with impaired CD8+ T cell proliferation to alloantigens (p = 0.002).
Conclusions: IPF as an indication for lung transplant is associated with short PBMC telomere length and impaired T cell responses to donor antigens. However, the rescue of proliferation following cytokine exposure suggests that alloimmune anergy could be overcome. Telomere length may inform immunosuppression strategies for IPF recipients.
Keywords: alloimmune response; idiopathic pulmonary fibrosis; immunosenescence; lung transplantation; telomeres.
Published by Elsevier Inc.
Figures



References
-
- Lederer DJ, Martinez FJ. Idiopathic Pulmonary Fibrosis. N Engl J Med 2018;378:1811–23. - PubMed
-
- Richeldi L, Collard HR, Jones MG. Idiopathic pulmonary fibrosis. Lancet 2017;389:1941–52. - PubMed
-
- George PM, Patterson CM, Reed AK, Thillai M. Lung transplantation for idiopathic pulmonary fibrosis. Lancet Respir Med 2019;7:271–82. - PubMed
-
- Blackburn EH, Epel ES, Lin J. Human telomere biology: A contributory and interactive factor in aging, disease risks, and protection. Science 2015;350:1193–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
