

Superiority of urgent vs early endoscopic hemostasis in patients with upper gastrointestinal bleeding with high-risk stigmata
- PMID: 34925851
- PMCID: PMC8677506
- DOI: 10.1093/gastro/goab042
Superiority of urgent vs early endoscopic hemostasis in patients with upper gastrointestinal bleeding with high-risk stigmata
Abstract
Background: Guidelines recommend that all patients with upper gastrointestinal bleeding (UGIB) undergo endoscopy within 24 h. It is unclear whether a subgroup may benefit from an urgent intervention. We aimed to evaluate the influence of endoscopic hemostasis and urgent endoscopy on mortality in UGIB patients with high-risk stigmata (HRS).
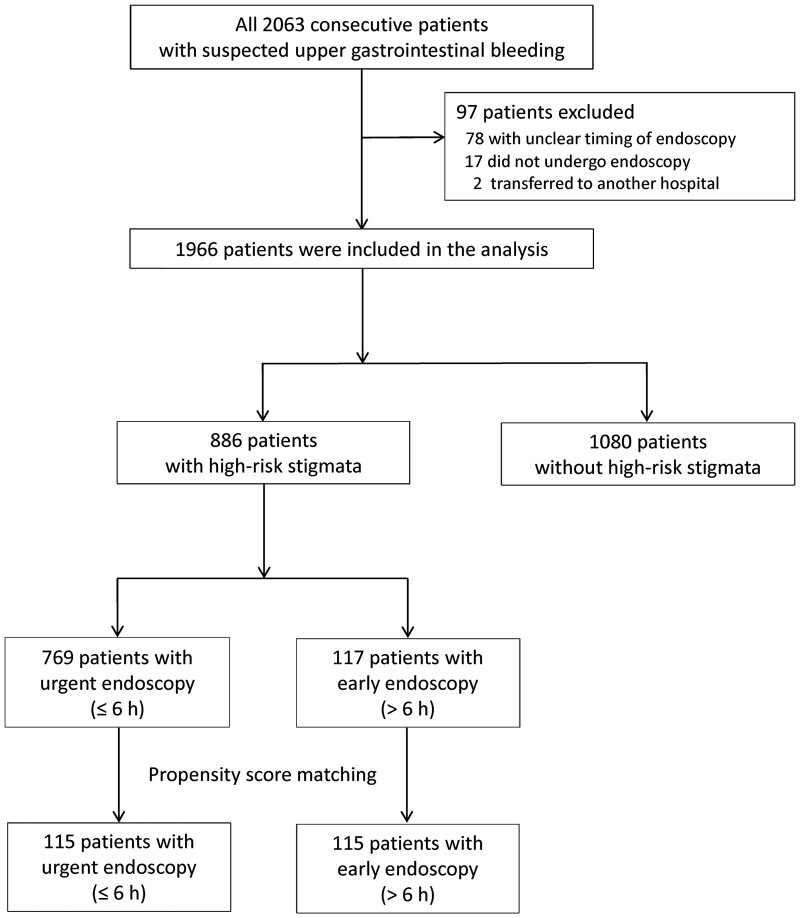
Methods: Consecutive patients with suspected UGIB were enrolled in three Japanese hospitals with a policy to perform endoscopy within 24 h. The primary outcome was 30-day mortality. Endoscopic hemostasis and endoscopy timing (urgent, ≤6 h; early, >6 h) were evaluated in a regression model adjusting for age, systolic pressure, heart rate, hemoglobin, creatinine, and variceal bleeding in multivariate analysis. A propensity score of 1:1 matched sensitivity analysis was also performed.
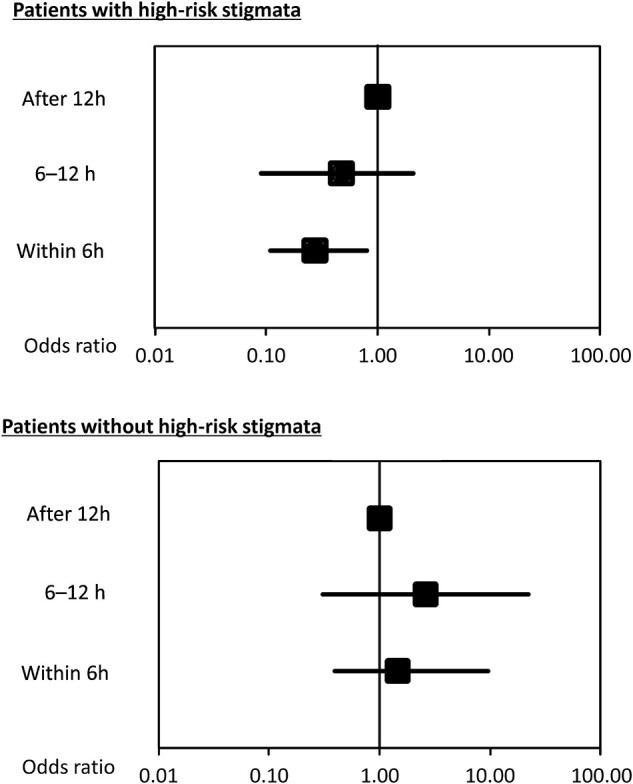
Results: HRS were present in 886 of 1966 patients, and 35 of 886 (3.95%) patients perished. Median urgent-endoscopy time (n = 769) was 3.0 h (interquartile range [IQR], 2.0-4.0 h) and early endoscopy (n = 117) was 12.0 h (IQR, 8.5-19.0 h). Successful endoscopic hemostasis and urgent endoscopy were significantly associated with reduced mortality in multivariable analysis (odds ratio [OR], 0.22; 95% confidence interval [CI], 0.09-0.52; P = 0.0006, and OR, 0.37; 95% CI, 0.16-0.87; P = 0.023, respectively). In a propensity-score-matched analysis of 115 pairs, adjusted comparisons showed significantly lower mortality of urgent vs early endoscopy (2.61% vs 7.83%, P < 0.001).
Conclusions: A subgroup of UGIB patients, namely those harboring HRS, may benefit from endoscopic hemostasis and urgent endoscopy rather than early endoscopy in reducing mortality. Implementing triage scores that predict the presence of such lesions is important.
Keywords: GBS; HARBINGER; UGIB; non-variceal bleeding; upper gastrointestinal bleeding; urgent endoscopy; variceal bleeding.
© The Author(s) 2021. Published by Oxford University Press and Sixth Affiliated Hospital of Sun Yat-sen University.
Figures
Similar articles
-
Urgent vs. non-urgent endoscopy in stable acute variceal bleeding.Am J Gastroenterol. 2009 May;104(5):1125-9. doi: 10.1038/ajg.2009.78. Epub 2009 Mar 31. Am J Gastroenterol. 2009. PMID: 19337243
-
Horibe GI bleeding prediction score: a simple score for triage decision-making in patients with suspected upper GI bleeding.Gastrointest Endosc. 2020 Sep;92(3):578-588.e4. doi: 10.1016/j.gie.2020.03.3846. Epub 2020 Mar 30. Gastrointest Endosc. 2020. PMID: 32240682
-
A simple scoring system to assess the need for an endoscopic intervention in suspected upper gastrointestinal bleeding: A prospective cohort study.Dig Liver Dis. 2016 Oct;48(10):1180-6. doi: 10.1016/j.dld.2016.07.009. Epub 2016 Jul 18. Dig Liver Dis. 2016. PMID: 27507771
-
AGA Clinical Practice Update on Endoscopic Therapies for Non-Variceal Upper Gastrointestinal Bleeding: Expert Review.Gastroenterology. 2020 Sep;159(3):1120-1128. doi: 10.1053/j.gastro.2020.05.095. Epub 2020 Jun 20. Gastroenterology. 2020. PMID: 32574620 Review.
-
Management of acute upper gastrointestinal bleeding: Urgent versus early endoscopy.Dig Endosc. 2022 Jan;34(2):260-264. doi: 10.1111/den.14144. Epub 2021 Oct 11. Dig Endosc. 2022. PMID: 34551156 Review.
Cited by
-
Acute Nonvariceal Upper Gastrointestinal Bleeding in Patients Using Anticoagulants: Does the Timing of Endoscopy Affect Outcomes?Dig Dis Sci. 2024 Feb;69(2):570-578. doi: 10.1007/s10620-023-08185-9. Epub 2023 Dec 20. Dig Dis Sci. 2024. PMID: 38117425 Free PMC article.
-
The Accuracy of Pre-Endoscopic Scores for Mortality Prediction in Patients with Upper GI Bleeding and No Endoscopy Performed.Diagnostics (Basel). 2023 Mar 21;13(6):1188. doi: 10.3390/diagnostics13061188. Diagnostics (Basel). 2023. PMID: 36980496 Free PMC article.
-
Does Early Endoscopy Affect the Clinical Outcomes of Patients with Acute Nonvariceal Upper Gastrointestinal Bleeding? A Systematic Review and Meta-Analysis.Gut Liver. 2023 Jul 15;17(4):566-580. doi: 10.5009/gnl220291. Epub 2022 Dec 29. Gut Liver. 2023. PMID: 36578195 Free PMC article.
-
Impact of duration to endoscopy in patients with non-variceal upper gastrointestinal bleeding: propensity score matching analysis of real-world data from Thailand.BMC Gastroenterol. 2025 Feb 17;25(1):86. doi: 10.1186/s12876-025-03673-w. BMC Gastroenterol. 2025. PMID: 39962393 Free PMC article.
References
-
- Laine L, Jensen DM. Management of patients with ulcer bleeding. Am J Gastroenterol 2012;107:345–60; quiz 61. - PubMed
-
- Hwang JH, Fisher DA, Ben-Menachem T et al.; Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. The role of endoscopy in the management of acute non-variceal upper GI bleeding. Gastrointest Endosc 2012;75:1132–8. - PubMed
-
- Heldwein W, Schreiner J, Pedrazzoli J et al. Is the Forrest classification a useful tool for planning endoscopic therapy of bleeding peptic ulcers? Endoscopy 1989;21:258–62. - PubMed
-
- Qureshi W, Adler DG, Davila R et al.; Standards of Practice Committee. ASGE Guideline: the role of endoscopy in the management of variceal hemorrhage, updated July 2005. Gastrointest Endosc 2005;62:651–5. - PubMed
LinkOut - more resources
Full Text Sources
