

Ventilation practices in burn patients-an international prospective observational cohort study
- PMID: 34926707
- PMCID: PMC8676707
- DOI: 10.1093/burnst/tkab034
Ventilation practices in burn patients-an international prospective observational cohort study
Abstract
Background: It is unknown whether lung-protective ventilation is applied in burn patients and whether they benefit from it. This study aimed to determine ventilation practices in burn intensive care units (ICUs) and investigate the association between lung-protective ventilation and the number of ventilator-free days and alive at day 28 (VFD-28).
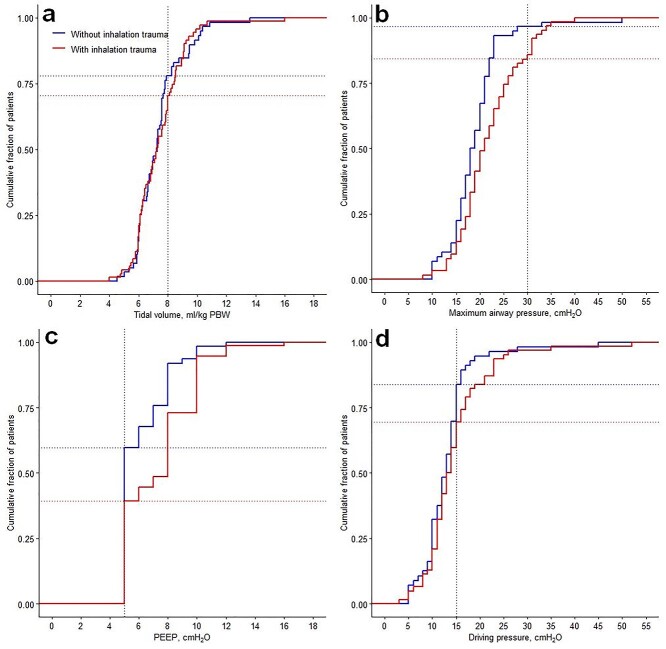
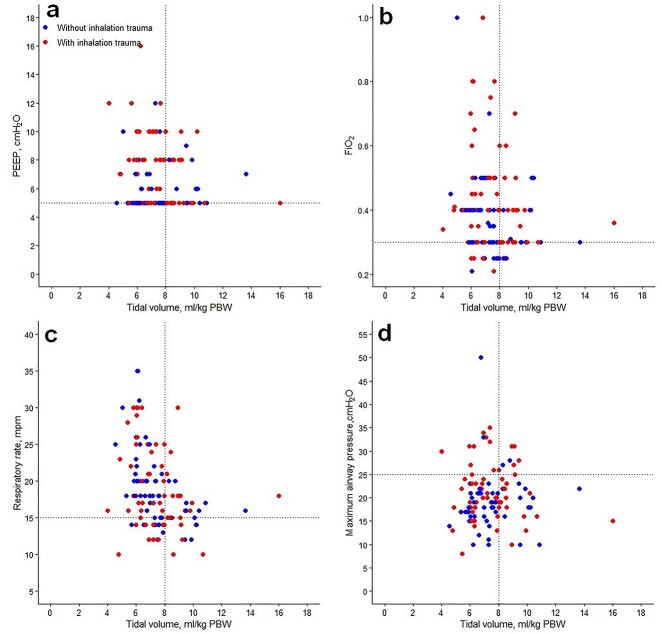
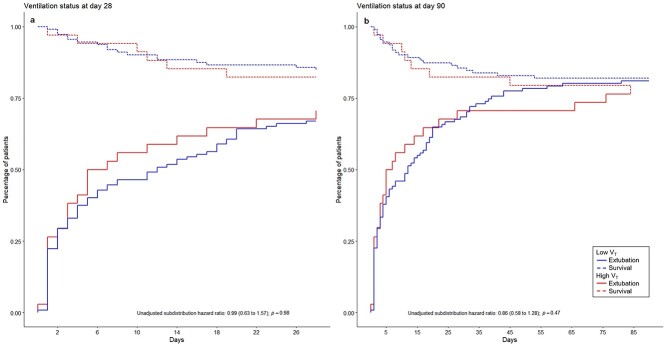
Methods: This is an international prospective observational cohort study including adult burn patients requiring mechanical ventilation. Low tidal volume (V T) was defined as V T ≤ 8 mL/kg predicted body weight (PBW). Levels of positive end-expiratory pressure (PEEP) and maximum airway pressures were collected. The association between V T and VFD-28 was analyzed using a competing risk model. Ventilation settings were presented for all patients, focusing on the first day of ventilation. We also compared ventilation settings between patients with and without inhalation trauma.
Results: A total of 160 patients from 28 ICUs in 16 countries were included. Low V T was used in 74% of patients, median V T size was 7.3 [interquartile range (IQR) 6.2-8.3] mL/kg PBW and did not differ between patients with and without inhalation trauma (p = 0.58). Median VFD-28 was 17 (IQR 0-26), without a difference between ventilation with low or high V T (p = 0.98). All patients were ventilated with PEEP levels ≥5 cmH2O; 80% of patients had maximum airway pressures <30 cmH2O.
Conclusion: In this international cohort study we found that lung-protective ventilation is used in the majority of burn patients, irrespective of the presence of inhalation trauma. Use of low V T was not associated with a reduction in VFD-28.
Trial registration: Clinicaltrials.gov NCT02312869. Date of registration: 9 December 2014.
Keywords: Critical care; Inhalation trauma; Lung-protective; Mechanical ventilation.
© The Author(s) 2021. Published by Oxford University Press.
Figures
References
-
- Fan E, Brodie D, Slutsky AS. Acute respiratory distress syndrome: advances in diagnosis and treatment. JAMA. 2018;319:698–710. - PubMed
-
- Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2014;370:980. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788–800. - PubMed
-
- Neto AS, Barbas CS, Simonis FD, Artigas-Raventos A, Canet J, Determann RM, et al. Epidemiological characteristics, practice of ventilation, and clinical outcome in patients at risk of acute respiratory distress syndrome in intensive care units from 16 countries (PRoVENT): an international, multicentre, prospective study. Lancet Respir Med. 2016;4:882–93. - PubMed
-
- Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The acute respiratory distress syndrome network. N Engl J Med. 2000;342:1301–8. - PubMed
