

Impact of Cardiac Arrest Centers on the Survival of Patients With Nontraumatic Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis
- PMID: 34927456
- PMCID: PMC9075197
- DOI: 10.1161/JAHA.121.023806
Impact of Cardiac Arrest Centers on the Survival of Patients With Nontraumatic Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis
Abstract
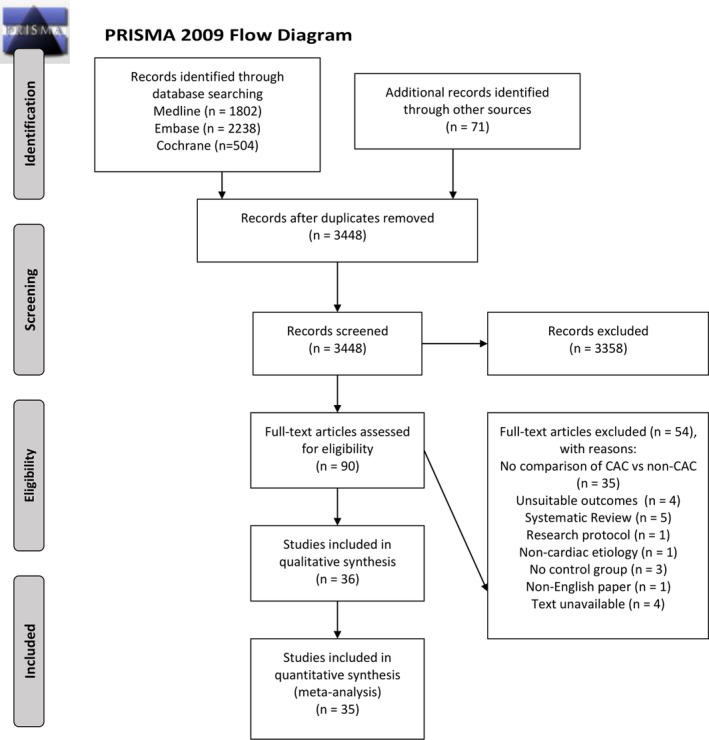
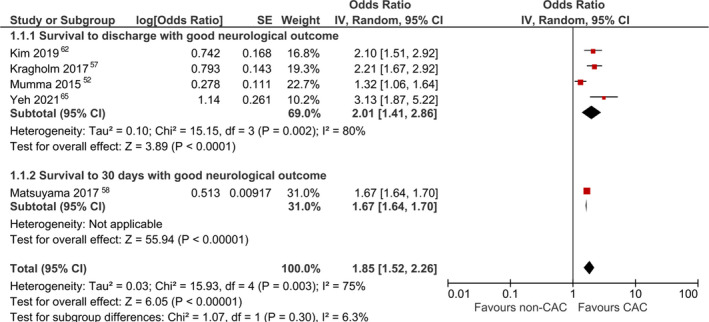
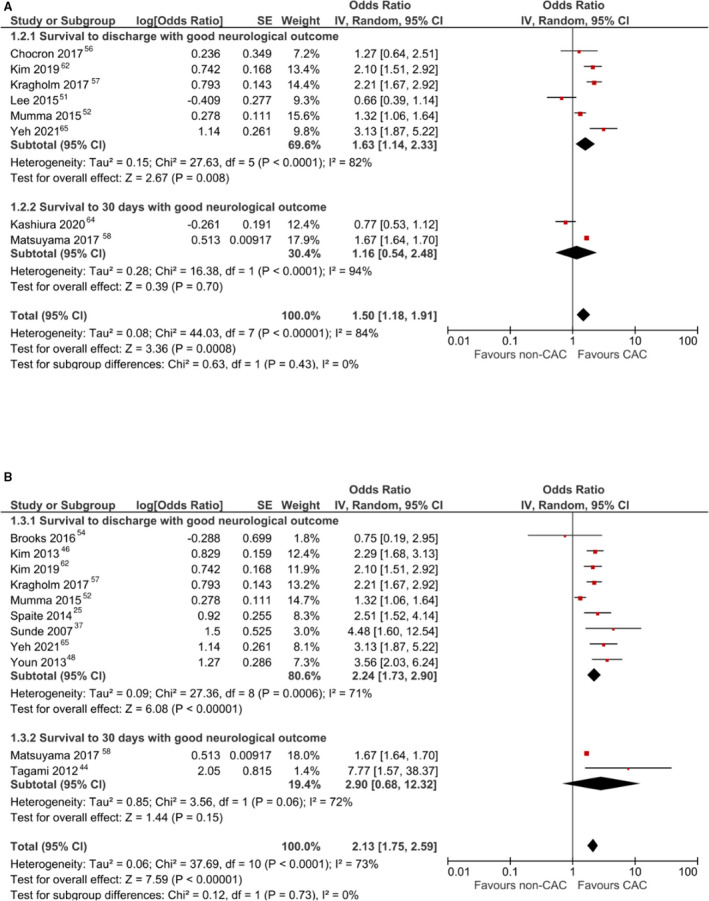
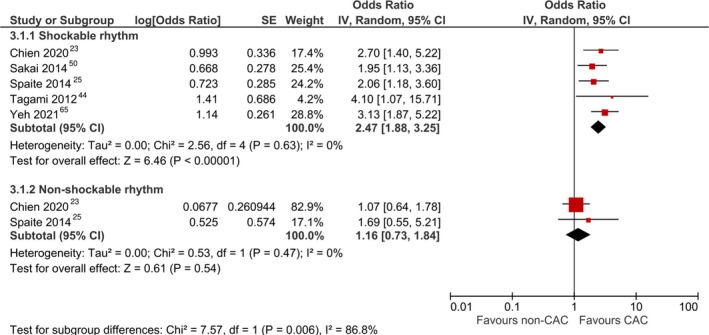
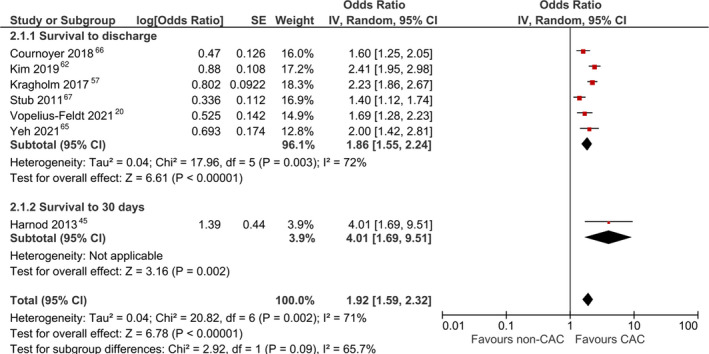
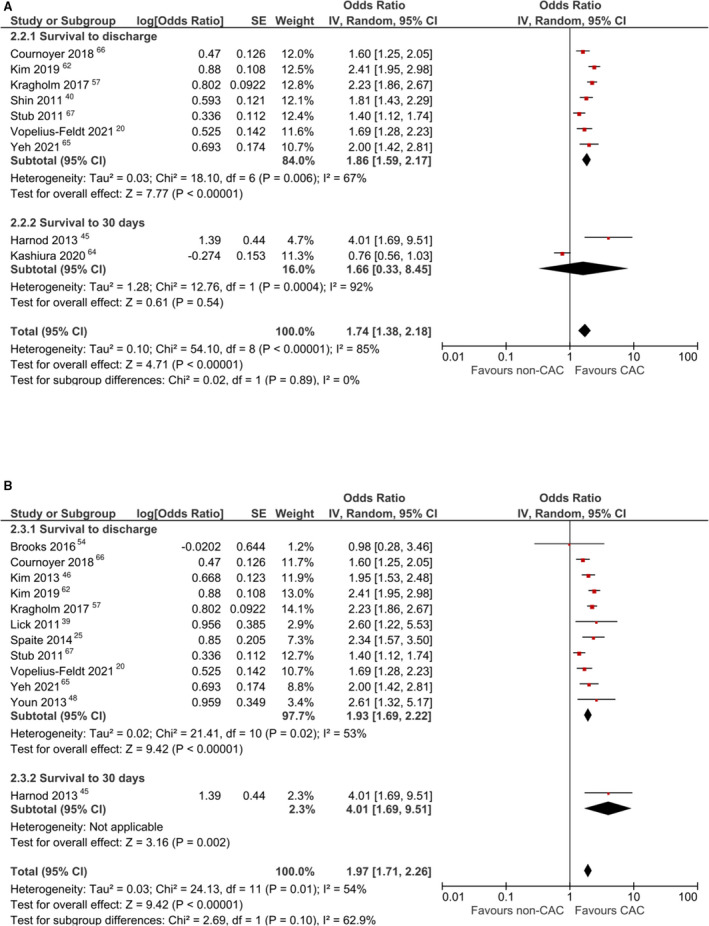
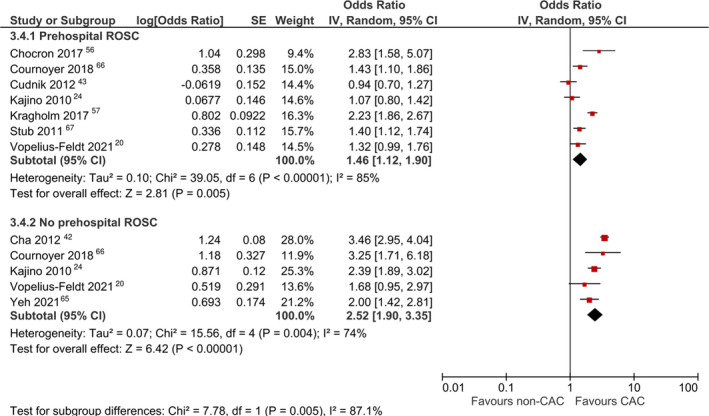
Background The role of cardiac arrest centers (CACs) in out-of-hospital cardiac arrest care systems is continuously evolving. Interpretation of existing literature is limited by heterogeneity in CAC characteristics and types of patients transported to CACs. This study assesses the impact of CACs on survival in out-of-hospital cardiac arrest according to varying definitions of CAC and prespecified subgroups. Methods and Results Electronic databases were searched from inception to March 9, 2021 for relevant studies. Centers were considered CACs if self-declared by study authors and capable of relevant interventions. Main outcomes were survival and neurologically favorable survival at hospital discharge or 30 days. Meta-analyses were performed for adjusted odds ratio (aOR) and crude odds ratios. Thirty-six studies were analyzed. Survival with favorable neurological outcome significantly improved with treatment at CACs (aOR, 1.85 [95% CI, 1.52-2.26]), even when including high-volume centers (aOR, 1.50 [95% CI, 1.18-1.91]) or including improved-care centers (aOR, 2.13 [95% CI, 1.75-2.59]) as CACs. Survival significantly increased with treatment at CACs (aOR, 1.92 [95% CI, 1.59-2.32]), even when including high-volume centers (aOR, 1.74 [95% CI, 1.38-2.18]) or when including improved-care centers (aOR, 1.97 [95% CI, 1.71-2.26]) as CACs. The treatment effect was more pronounced among patients with shockable rhythm (P=0.006) and without prehospital return of spontaneous circulation (P=0.005). Conclusions were robust to sensitivity analyses, with no publication bias detected. Conclusions Care at CACs was associated with improved survival and neurological outcomes for patients with nontraumatic out-of-hospital cardiac arrest regardless of varying CAC definitions. Patients with shockable rhythms and those without prehospital return of spontaneous circulation benefited more from CACs. Evidence for bypassing hospitals or interhospital transfer remains inconclusive.
Keywords: cardiac arrest; cardiac arrest center; heart arrest; resuscitation.
Figures
References
-
- Kiguchi T, Okubo M, Nishiyama C, Maconochie I, Ong MEH, Kern KB, Wyckoff MH, McNally B, Christensen EF, Tjelmeland I, et al. Out‐of‐hospital cardiac arrest across the world: first report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation. 2020;152:39–49. doi: 10.1016/j.resuscitation.2020.02.044 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
