

Effect of Regional vs General Anesthesia on Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery: The RAGA Randomized Trial
- PMID: 34928310
- PMCID: PMC8689436
- DOI: 10.1001/jama.2021.22647
Effect of Regional vs General Anesthesia on Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery: The RAGA Randomized Trial
Erratum in
-
Incorrect Values in Tables.JAMA. 2022 Mar 22;327(12):1188. doi: 10.1001/jama.2022.3565. JAMA. 2022. PMID: 35315908 Free PMC article. No abstract available.
Abstract
Importance: In adults undergoing hip fracture surgery, regional anesthesia may reduce postoperative delirium, but there is uncertainty about its effectiveness.
Objective: To investigate, in older adults undergoing surgical repair for hip fracture, the effects of regional anesthesia on the incidence of postoperative delirium compared with general anesthesia.
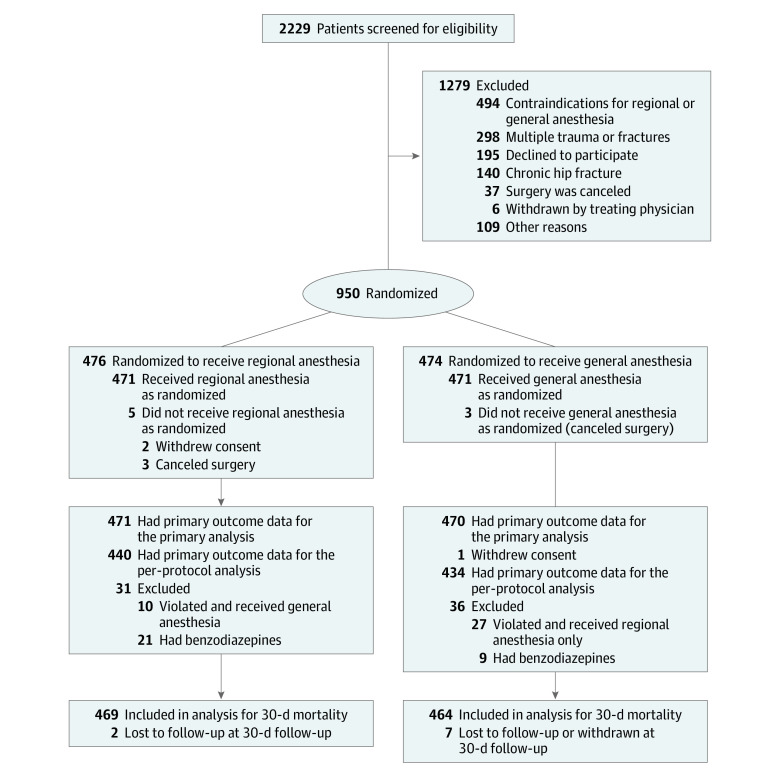
Design, setting, and participants: A randomized, allocation-concealed, open-label, multicenter clinical trial of 950 patients, aged 65 years and older, with or without preexisting dementia, and a fragility hip fracture requiring surgical repair from 9 university teaching hospitals in Southeastern China. Participants were enrolled between October 2014 and September 2018; 30-day follow-up ended November 2018.
Interventions: Patients were randomized to receive either regional anesthesia (spinal, epidural, or both techniques combined with no sedation; n = 476) or general anesthesia (intravenous, inhalational, or combined anesthetic agents; n = 474).
Main outcomes and measures: Primary outcome was incidence of delirium during the first 7 postoperative days. Secondary outcomes analyzed in this article include delirium severity, duration, and subtype; postoperative pain score; length of hospitalization; 30-day all-cause mortality; and complications.
Results: Among 950 randomized patients (mean age, 76.5 years; 247 [26.8%] male), 941 were evaluable for the primary outcome (6 canceled surgery and 3 withdrew consent). Postoperative delirium occurred in 29 (6.2%) in the regional anesthesia group vs 24 (5.1%) in the general anesthesia group (unadjusted risk difference [RD], 1.1%; 95% CI, -1.7% to 3.8%; P = .48; unadjusted relative risk [RR], 1.2 [95% CI, 0.7 to 2.0]; P = .57]). Mean severity score of delirium was 23.0 vs 24.1, respectively (unadjusted difference, -1.1; 95% CI, -4.6 to 3.1). A single delirium episode occurred in 16 (3.4%) vs 10 (2.1%) (unadjusted RD, 1.1%; 95% CI, -1.7% to 3.9%; RR, 1.6 [95% CI, 0.7 to 3.5]). Hypoactive subtype in 11 (37.9%) vs 5 (20.8%) (RD, 11.5; 95% CI, -11.0% to 35.7%; RR, 2.2 [95% CI, 0.8 to 6.3]). Median worst pain score was 0 (IQR, 0 to 20) vs 0 (IQR, 0 to 10) (difference 0; 95% CI, 0 to 0). Median length of hospitalization was 7 days (IQR, 5 to 10) vs 7 days (IQR, 6 to 10) (difference 0; 95% CI, 0 to 0). Death occurred in 8 (1.7%) vs 4 (0.9%) (unadjusted RD, -0.8%; 95% CI, -2.2% to 0.7%; RR, 2.0 [95% CI, 0.6 to 6.5]). Adverse events were reported in 106 episodes in the regional anesthesia group and 102 in the general anesthesia group; the most frequently reported adverse events were nausea and vomiting (47 [44.3%] vs 34 [33.3%]) and postoperative hypotension (13 [12.3%] vs 10 [9.8%]).
Conclusions and relevance: In patients aged 65 years and older undergoing hip fracture surgery, regional anesthesia without sedation did not significantly reduce the incidence of postoperative delirium compared with general anesthesia.
Trial registration: ClinicalTrials.gov Identifier: NCT02213380.
Conflict of interest statement
Figures
Comment in
-
General Anesthesia and Postoperative Neurocognitive Outcomes.JAMA. 2022 Jan 4;327(1):36-38. doi: 10.1001/jama.2021.22465. JAMA. 2022. PMID: 34928317 Free PMC article. No abstract available.
-
[Is delirium independent from the anesthesia technique?-What REGAIN and RAGA teach us].Anaesthesist. 2022 May;71(5):400-402. doi: 10.1007/s00101-022-01104-z. Epub 2022 Feb 23. Anaesthesist. 2022. PMID: 35199183 Free PMC article. German. No abstract available.
-
In older adults having hip fracture surgery, regional vs. general anesthesia did not reduce postoperative delirium.Ann Intern Med. 2022 May;175(5):JC53. doi: 10.7326/J22-0027. Epub 2022 May 3. Ann Intern Med. 2022. PMID: 35500260
-
Regional vs General Anesthesia and Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery.JAMA. 2022 May 3;327(17):1708. doi: 10.1001/jama.2022.3541. JAMA. 2022. PMID: 35503351 No abstract available.
-
Regional vs General Anesthesia and Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery.JAMA. 2022 May 3;327(17):1707-1708. doi: 10.1001/jama.2022.3538. JAMA. 2022. PMID: 35503352 No abstract available.
-
Regional vs General Anesthesia and Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery.JAMA. 2022 May 3;327(17):1707. doi: 10.1001/jama.2022.3535. JAMA. 2022. PMID: 35503353 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
