

Responses to a Neutralizing Monoclonal Antibody for Hospitalized Patients With COVID-19 According to Baseline Antibody and Antigen Levels : A Randomized Controlled Trial
- PMID: 34928698
- PMCID: PMC9334931
- DOI: 10.7326/M21-3507
Responses to a Neutralizing Monoclonal Antibody for Hospitalized Patients With COVID-19 According to Baseline Antibody and Antigen Levels : A Randomized Controlled Trial
Abstract
Background: In a randomized, placebo-controlled, clinical trial, bamlanivimab, a SARS-CoV-2-neutralizing monoclonal antibody, given in combination with remdesivir, did not improve outcomes among hospitalized patients with COVID-19 based on an early futility assessment.
Objective: To evaluate the a priori hypothesis that bamlanivimab has greater benefit in patients without detectable levels of endogenous neutralizing antibody (nAb) at study entry than in those with antibodies, especially if viral levels are high.
Design: Randomized, placebo-controlled trial. (ClinicalTrials.gov: NCT04501978).
Setting: Multicenter trial.
Patients: Hospitalized patients with COVID-19 without end-organ failure.
Intervention: Bamlanivimab (7000 mg) or placebo.
Measurements: Antibody, antigen, and viral RNA levels were centrally measured on stored specimens collected at baseline. Patients were followed for 90 days for sustained recovery (defined as discharge to home and remaining home for 14 consecutive days) and a composite safety outcome (death, serious adverse events, organ failure, or serious infections).
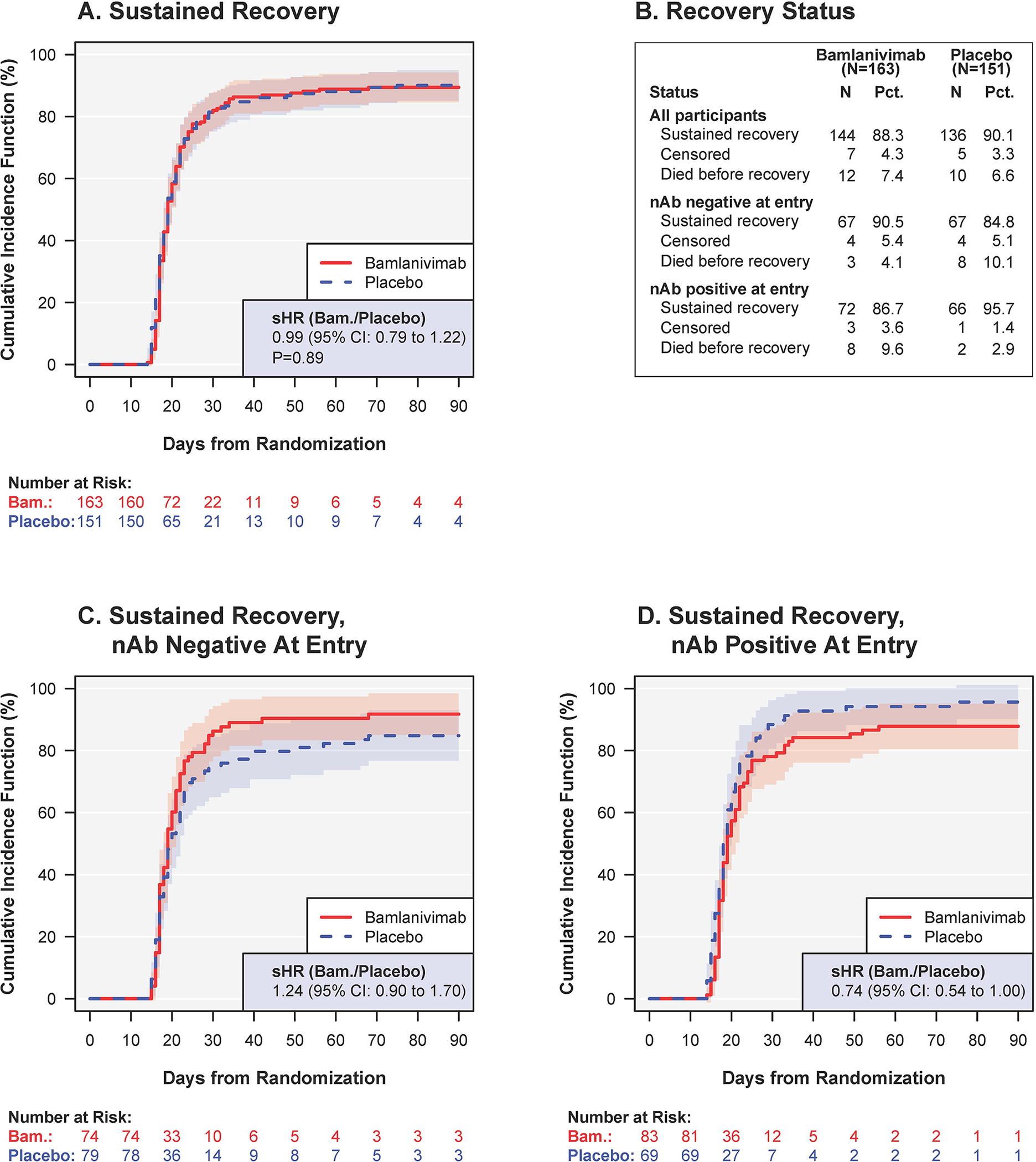
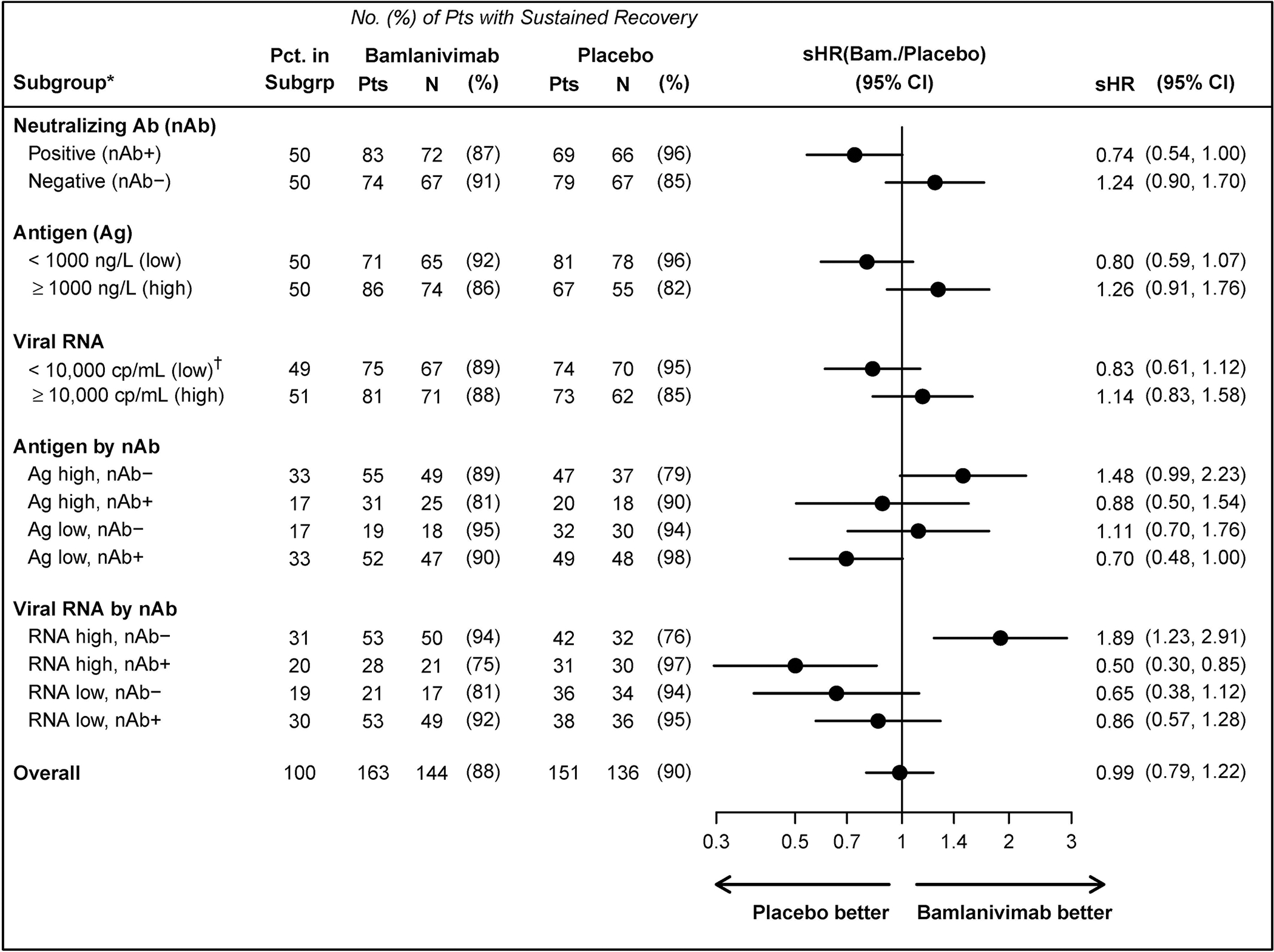
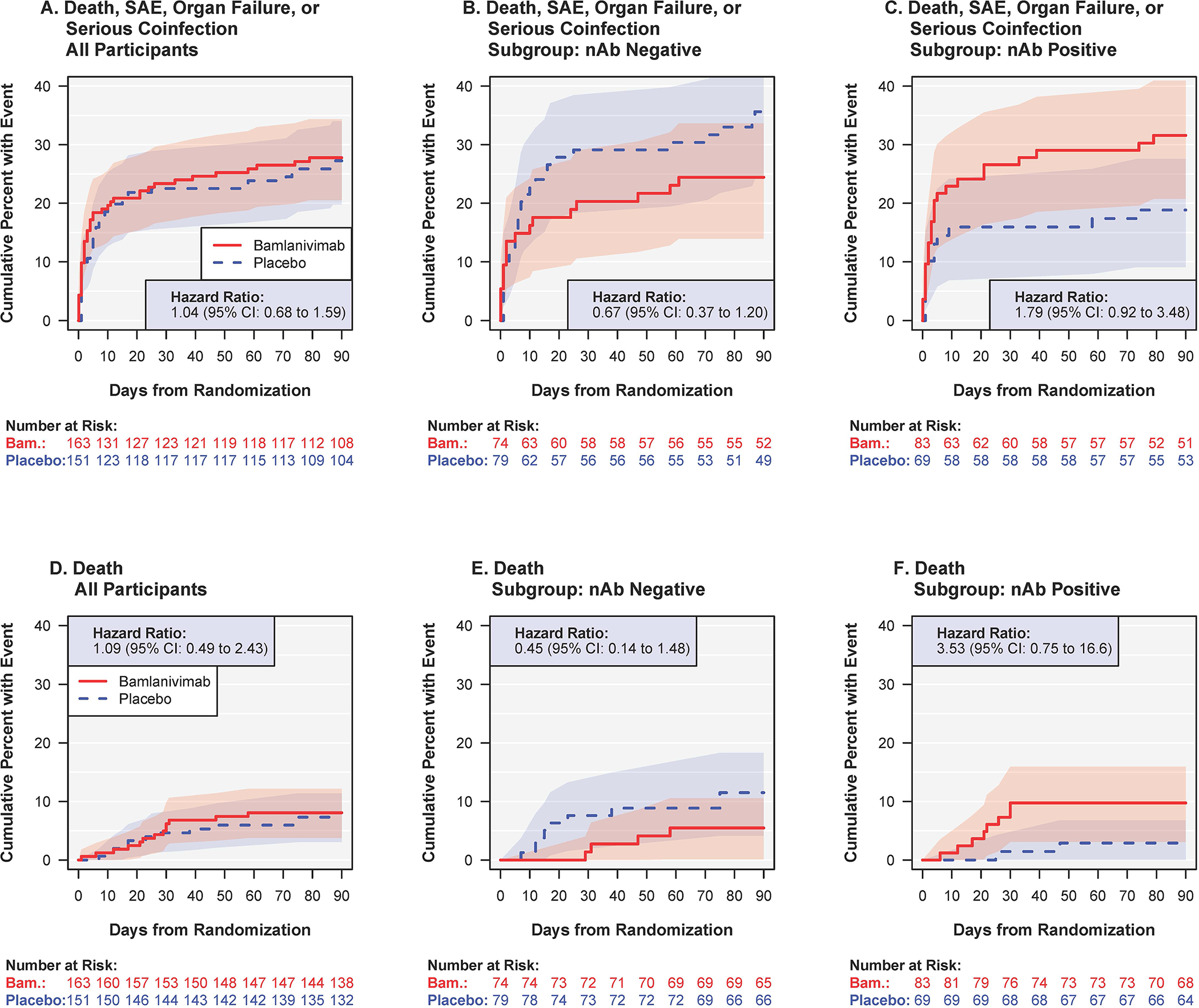
Results: Among 314 participants (163 receiving bamlanivimab and 151 placebo), the median time to sustained recovery was 19 days and did not differ between the bamlanivimab and placebo groups (subhazard ratio [sHR], 0.99 [95% CI, 0.79 to 1.22]; sHR > 1 favors bamlanivimab). At entry, 50% evidenced production of anti-spike nAbs; 50% had SARS-CoV-2 nucleocapsid plasma antigen levels of at least 1000 ng/L. Among those without and with nAbs at study entry, the sHRs were 1.24 (CI, 0.90 to 1.70) and 0.74 (CI, 0.54 to 1.00), respectively (nominal P for interaction = 0.018). The sHR (bamlanivimab vs. placebo) was also more than 1 for those with plasma antigen or nasal viral RNA levels above median level at entry and was greatest for those without antibodies and with elevated levels of antigen (sHR, 1.48 [CI, 0.99 to 2.23]) or viral RNA (sHR, 1.89 [CI, 1.23 to 2.91]). Hazard ratios for the composite safety outcome (<1 favors bamlanivimab) also differed by serostatus at entry: 0.67 (CI, 0.37 to 1.20) for those without and 1.79 (CI, 0.92 to 3.48) for those with nAbs.
Limitation: Subgroup analysis of a trial prematurely stopped because of futility; small sample size; multiple subgroups analyzed.
Conclusion: Efficacy and safety of bamlanivimab may differ depending on whether an endogenous nAb response has been mounted. The limited sample size of the study does not allow firm conclusions based on these findings, and further independent trials are required that assess other types of passive immune therapies in the same patient setting.
Primary funding source: U.S. government Operation Warp Speed and National Institute of Allergy and Infectious Diseases.
Figures
References
-
- Gupta A, Gonzalez-Rojas Y, Juarez E, Casal MC, Moya J, Falci DR, et al. Early Covid-19 Treatment With SARS-CoV-2 Neutralizing Antibody Sotrovimab. medRxiv. 2021:2021.05.27.21257096. - PubMed
-
- O’Brien MP, Forleo Neto E, Chen KC, Isa F, Heirman I, Sarkar N, et al. Casirivimab with Imdevimab antibody cocktail for COVID-19 prevention: interim results. CROI 2021.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous