

Access to and safety of COVID-19 convalescent plasma in the United States Expanded Access Program: A national registry study
- PMID: 34928960
- PMCID: PMC8730442
- DOI: 10.1371/journal.pmed.1003872
Access to and safety of COVID-19 convalescent plasma in the United States Expanded Access Program: A national registry study
Abstract
Background: The United States (US) Expanded Access Program (EAP) to coronavirus disease 2019 (COVID-19) convalescent plasma was initiated in response to the rapid spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of COVID-19. While randomized clinical trials were in various stages of development and enrollment, there was an urgent need for widespread access to potential therapeutic agents. The objective of this study is to report on the demographic, geographical, and chronological characteristics of patients in the EAP, and key safety metrics following transfusion of COVID-19 convalescent plasma.
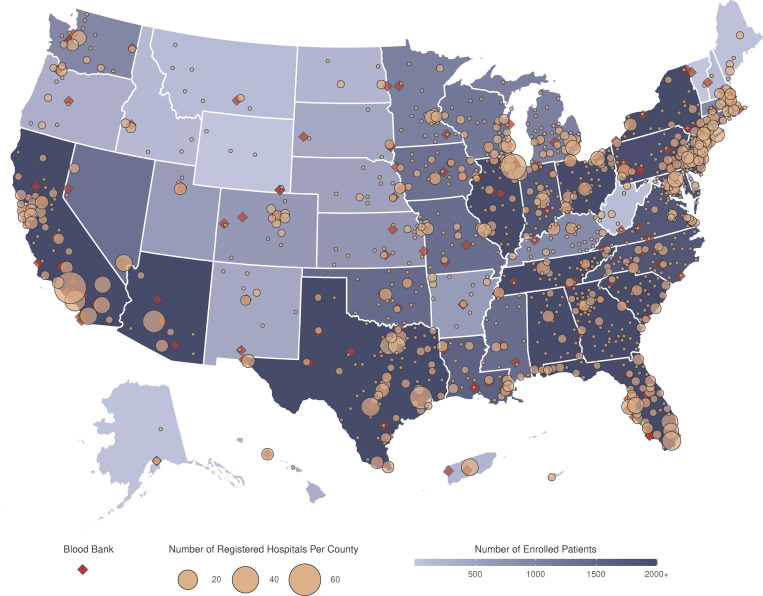
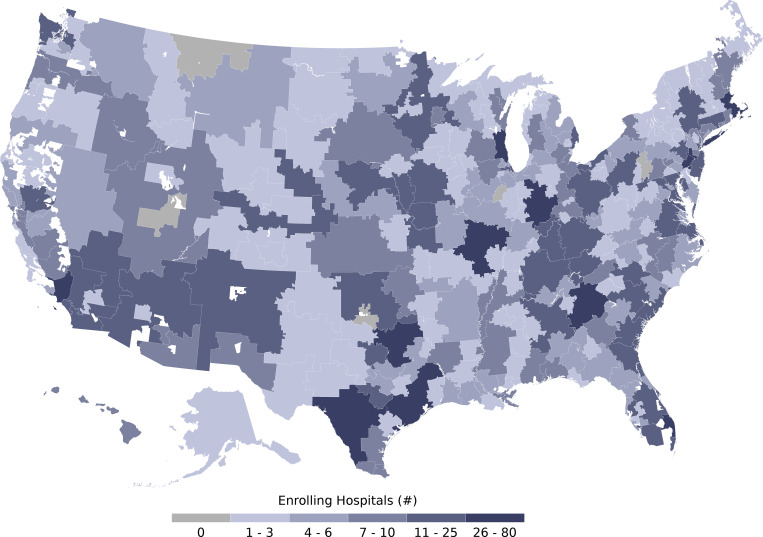
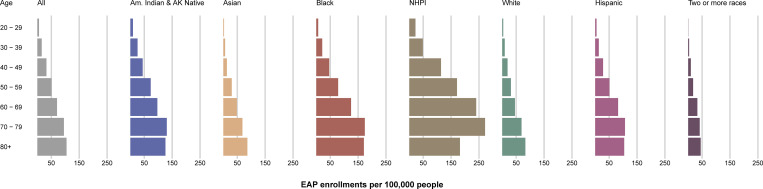
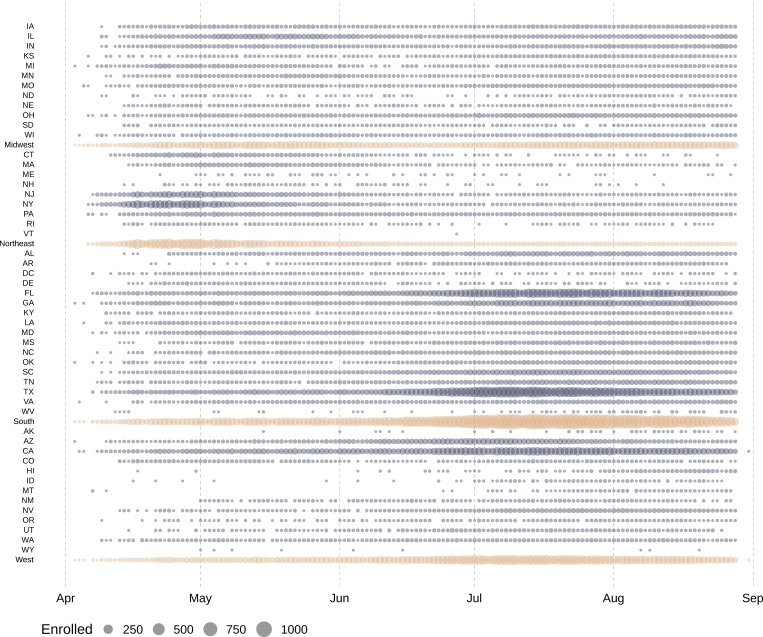
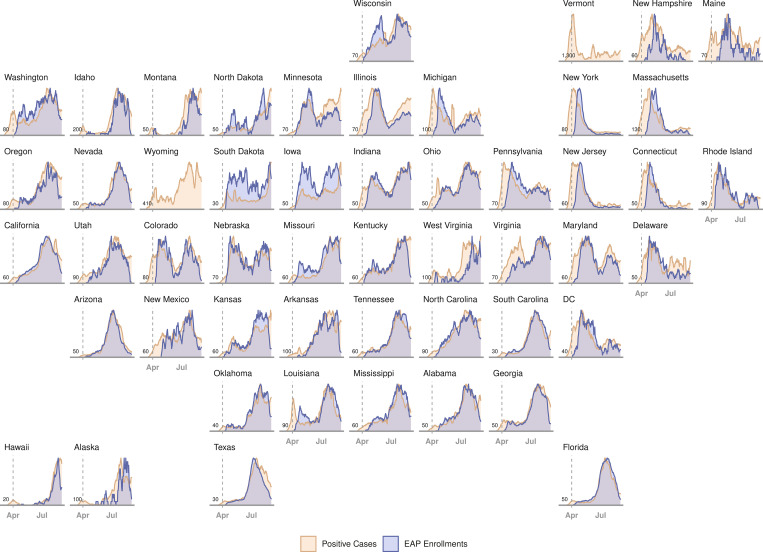
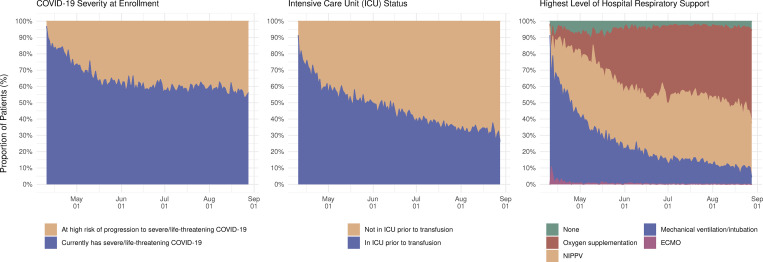
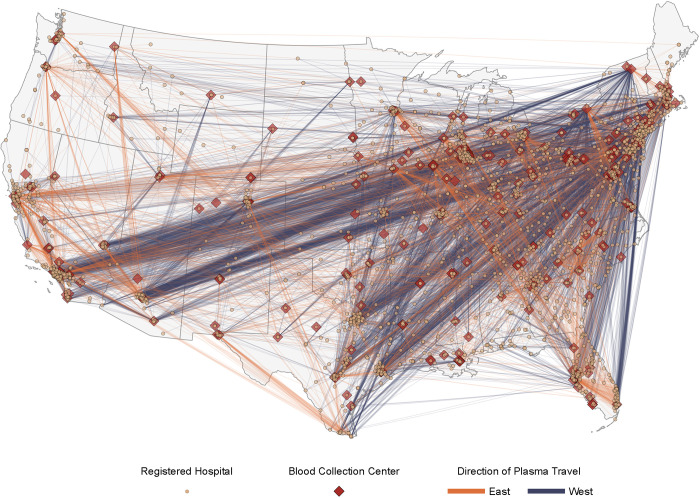
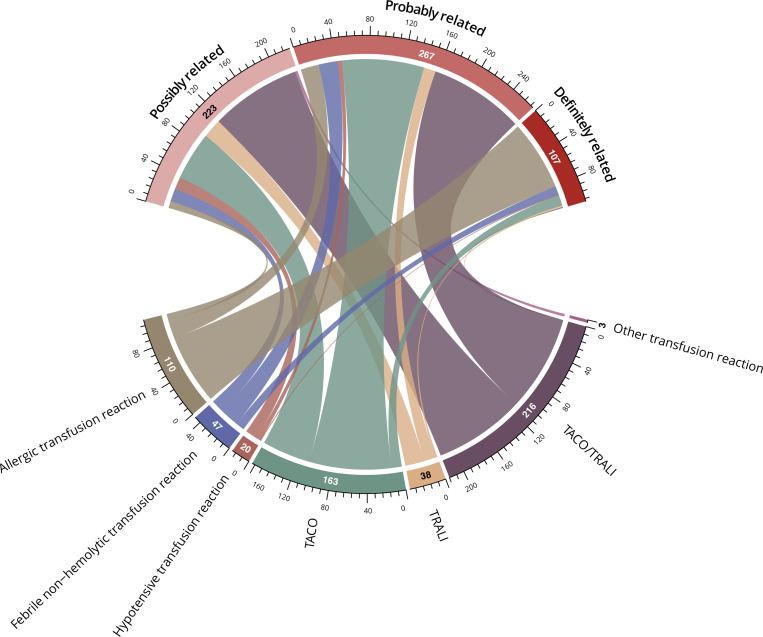
Methods and findings: Mayo Clinic served as the central institutional review board for all participating facilities, and any US physician could participate as a local physician-principal investigator. Eligible patients were hospitalized, were aged 18 years or older, and had-or were at risk of progression to-severe or life-threatening COVID-19; eligible patients were enrolled through the EAP central website. Blood collection facilities rapidly implemented programs to collect convalescent plasma for hospitalized patients with COVID-19. Demographic and clinical characteristics of all enrolled patients in the EAP were summarized. Temporal patterns in access to COVID-19 convalescent plasma were investigated by comparing daily and weekly changes in EAP enrollment in response to changes in infection rate at the state level. Geographical analyses on access to convalescent plasma included assessing EAP enrollment in all national hospital referral regions, as well as assessing enrollment in metropolitan areas and less populated areas that did not have access to COVID-19 clinical trials. From April 3 to August 23, 2020, 105,717 hospitalized patients with severe or life-threatening COVID-19 were enrolled in the EAP. The majority of patients were 60 years of age or older (57.8%), were male (58.4%), and had overweight or obesity (83.8%). There was substantial inclusion of minorities and underserved populations: 46.4% of patients were of a race other than white, and 37.2% of patients were of Hispanic ethnicity. Chronologically and geographically, increases in the number of both enrollments and transfusions in the EAP closely followed confirmed infections across all 50 states. Nearly all national hospital referral regions enrolled and transfused patients in the EAP, including both in metropolitan and in less populated areas. The incidence of serious adverse events was objectively low (<1%), and the overall crude 30-day mortality rate was 25.2% (95% CI, 25.0% to 25.5%). This registry study was limited by the observational and pragmatic study design that did not include a control or comparator group; thus, the data should not be used to infer definitive treatment effects.
Conclusions: These results suggest that the EAP provided widespread access to COVID-19 convalescent plasma in all 50 states, including for underserved racial and ethnic minority populations. The study design of the EAP may serve as a model for future efforts when broad access to a treatment is needed in response to an emerging infectious disease.
Trial registration: ClinicalTrials.gov NCT#: NCT04338360.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Update of
-
Program and patient characteristics for the United States Expanded Access Program to COVID-19 convalescent plasma.medRxiv [Preprint]. 2021 Apr 10:2021.04.08.21255115. doi: 10.1101/2021.04.08.21255115. medRxiv. 2021. Update in: PLoS Med. 2021 Dec 20;18(12):e1003872. doi: 10.1371/journal.pmed.1003872. PMID: 33851175 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
