

Anterior Cruciate Ligament Reconstruction versus Nonoperative Treatment: Better Function and Less Secondary Meniscectomies But No Difference in Knee Osteoarthritis-A Meta-Analysis
- PMID: 34929763
- PMCID: PMC8808919
- DOI: 10.1177/19476035211046041
Anterior Cruciate Ligament Reconstruction versus Nonoperative Treatment: Better Function and Less Secondary Meniscectomies But No Difference in Knee Osteoarthritis-A Meta-Analysis
Abstract
Objectives: The impact of anterior cruciate ligament (ACL) reconstruction on knee osteoarthritis (OA) is still unclear. The aim of the current meta-analysis was to compare surgical treatment versus nonoperative management of ACL tears to assess the impact of these approaches on knee OA development at a 5 and 10 years of follow-up.
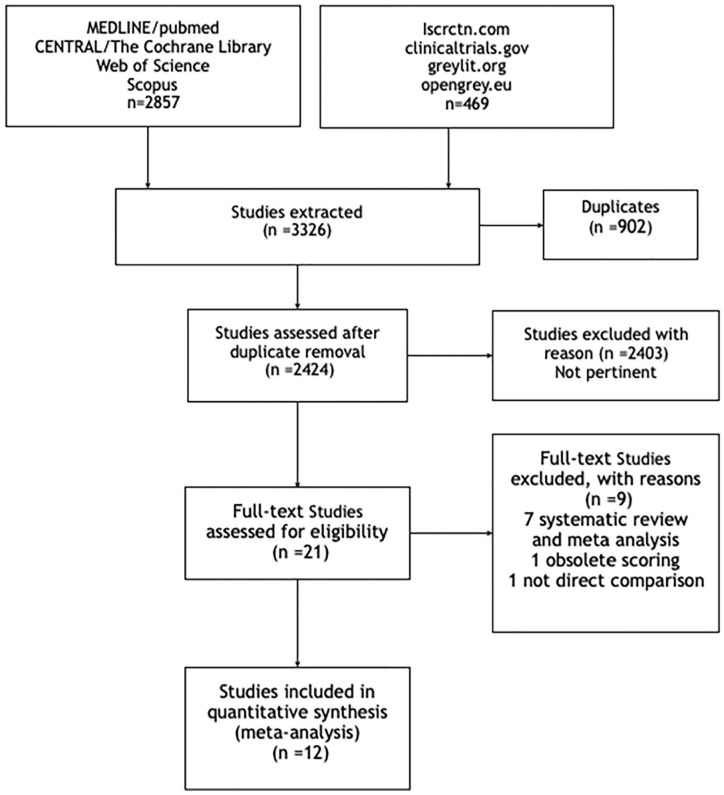
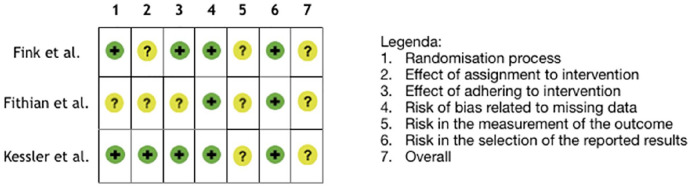
Design: A meta-analysis was performed after a systematic literature search (May 2021) was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. Both randomized and nonrandomized comparative studies with more than 5 years of follow-up were selected. Influence of the treatment was assessed in terms of knee OA development, subjective and objective clinical results, activity level, and risk of further surgeries. Risk of bias and quality of evidence were assessed following the Cochrane guidelines.
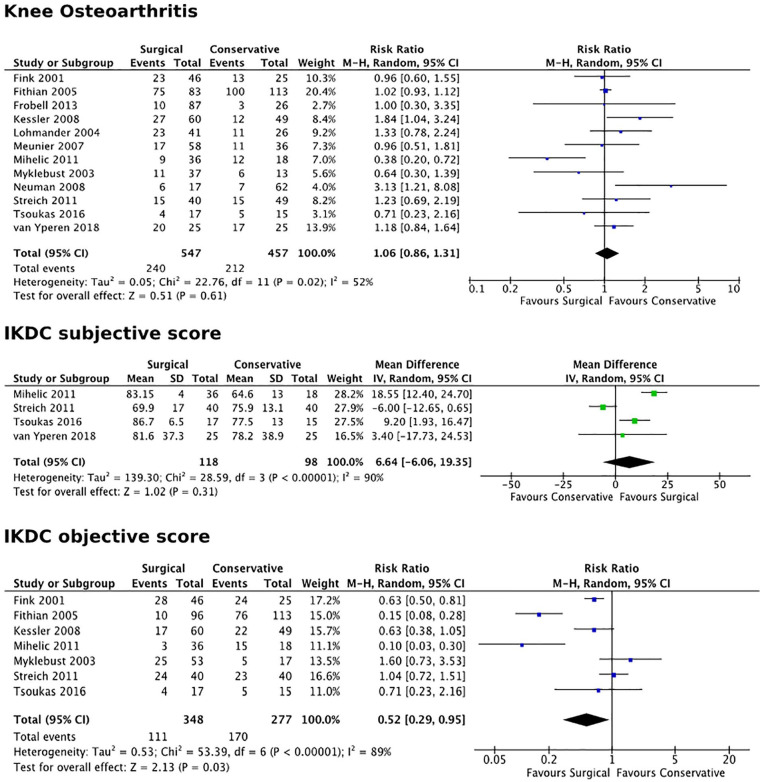
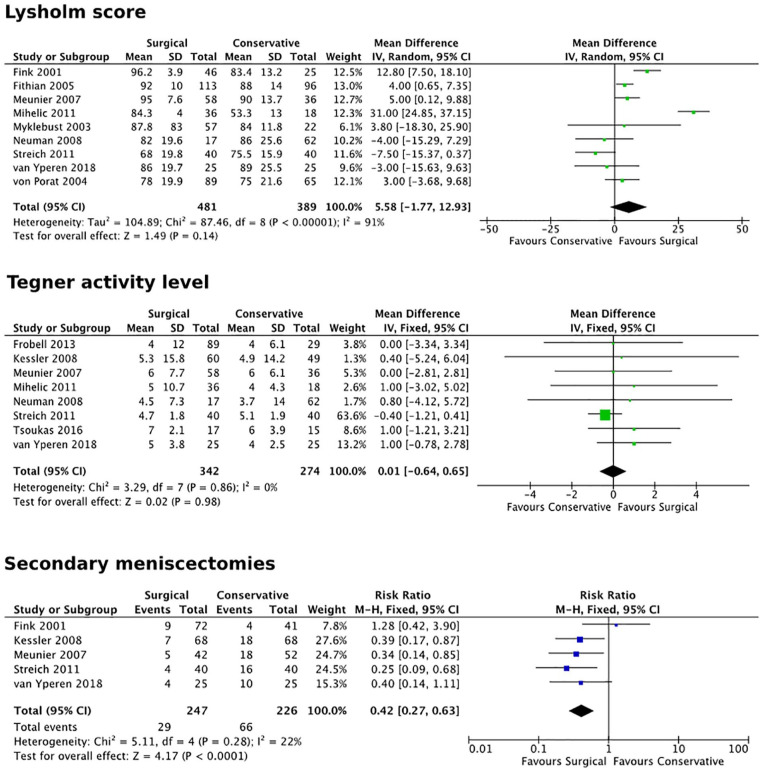
Results: Twelve studies matched the inclusion criteria, for a total of 1,004 patients. Level of evidence was rated low to very low. No difference was documented in terms of knee OA development, Tegner score, subjective International Knee Documentation Committee (IKDC), and Lysholm scores. A significant difference favoring the surgical treatment in comparison with a nonsurgical approach was observed in terms of objective IKDC score (P = 0.03) and risk of secondary meniscectomy (P < 0.0001). The level of evidence was considered very low for subjective IKDC, low for knee OA development, objective IKDC, number of secondary meniscectomies, and Lysholm score, and moderate for post-op Tegner score.
Conclusions: The meta-analysis did not support an advantage of ACL reconstruction in terms of OA prevention in comparison with a nonoperative treatment. Moreover, no differences were reported for subjective results and activity level at 5 and 10 years of follow-up. On the contrary, patients who underwent surgical treatment of their ACL tear presented important clinical findings in terms of better objective knee function and a lower rate of secondary meniscectomies when compared with conservatively managed patents.Protocol Registration: CRD420191156483 (PROSPERO).
Keywords: ACL reconstruction; anterior cruciate ligament; conservative treatment; osteoarthritis; radiologic evaluation.
Conflict of interest statement
Figures
 )
stands for “low risk”; yellow (
)
stands for “low risk”; yellow ( ) for “moderate
risk”; red for (
) for “moderate
risk”; red for ( ) “high risk.”
) “high risk.”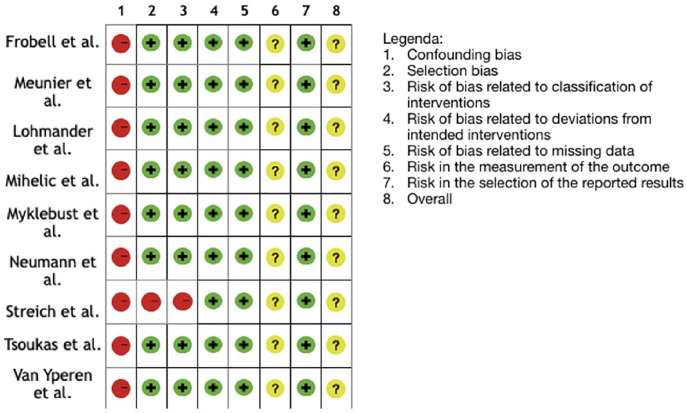 )
stands for “low risk”; yellow () for “moderate
risk”; red for () “high risk.”
)
stands for “low risk”; yellow () for “moderate
risk”; red for () “high risk.”References
-
- Gianotti SM, Marshall SW, Hume PA, Bunt L. Incidence of anterior cruciate ligament injury and other knee ligament injuries: a national population-based study. J Sci Med Sport. 2009;12(6): 622-7. - PubMed
-
- Lyman S, Koulouvaris P, Sherman S, Do H, Mandl LA, Marx RG. Epidemiology of anterior cruciate ligament reconstruction: trends, readmissions, and subsequent knee surgery. J Bone Joint Surg Am. 2009;91(10): 2321-8. - PubMed
-
- Majewski M, Susanne H, Klaus S. Epidemiology of athletic knee injuries: a 10-year study. Knee. 2006;13(3): 184-8. - PubMed
-
- Mall NA, Chalmers PN, Moric M, Tanaka MJ, Cole BJ, Bach BR, Jr, et al.. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42(10): 2363-70. - PubMed
-
- Sanders TL, Maradit Kremers H, Bryan AJ, Larson DR, Dahm DL, Levy BA, et al.. Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med. 2016;44(6): 1502-7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
