

Haematological response in experimental human Plasmodium falciparum and Plasmodium vivax malaria
- PMID: 34930260
- PMCID: PMC8685492
- DOI: 10.1186/s12936-021-04003-7
Haematological response in experimental human Plasmodium falciparum and Plasmodium vivax malaria
Abstract
Background: Malaria-associated anaemia, arising from symptomatic, asymptomatic and submicroscopic infections, is a significant cause of morbidity worldwide. Induced blood stage malaria volunteer infection studies (IBSM-VIS) provide a unique opportunity to evaluate the haematological response to early Plasmodium falciparum and Plasmodium vivax infection.
Methods: This study was an analysis of the haemoglobin, red cell counts, and parasitaemia data from 315 participants enrolled in IBSM-VIS between 2012 and 2019, including 269 participants inoculated with the 3D7 strain of P. falciparum (Pf3D7), 15 with an artemisinin-resistant P. falciparum strain (PfK13) and 46 with P. vivax. Factors associated with the fractional fall in haemoglobin (Hb-FF) were evaluated, and the malaria-attributable erythrocyte loss after accounting for phlebotomy-related losses was estimated. The relative contribution of parasitized erythrocytes to the malaria-attributable erythrocyte loss was also estimated.
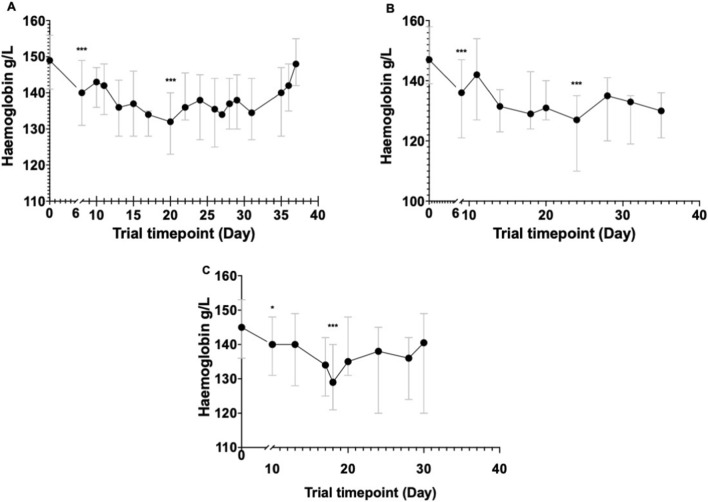
Results: The median peak parasitaemia prior to treatment was 10,277 parasites/ml (IQR 3566-27,815), 71,427 parasites/ml [IQR 33,236-180,213], and 34,840 parasites/ml (IQR 13,302-77,064) in participants inoculated with Pf3D7, PfK13, and P. vivax, respectively. The median Hb-FF was 10.3% (IQR 7.8-13.3), 14.8% (IQR 11.8-15.9) and 11.7% (IQR 8.9-14.5) in those inoculated with Pf3D7, PfK13 and P. vivax, respectively, with the haemoglobin nadir occurring a median 12 (IQR 5-21), 15 (IQR 7-22), and 8 (IQR 7-15) days following inoculation. In participants inoculated with P. falciparum, recrudescence was associated with a greater Hb-FF, while in those with P. vivax, the Hb-FF was associated with a higher pre-treatment parasitaemia and later day of anti-malarial treatment. After accounting for phlebotomy-related blood losses, the estimated Hb-FF was 4.1% (IQR 3.1-5.3), 7.2% (IQR 5.8-7.8), and 4.9% (IQR 3.7-6.1) in participants inoculated with Pf3D7, PfK13, and P. vivax, respectively. Parasitized erythrocytes were estimated to account for 0.015% (IQR 0.006-0.06), 0.128% (IQR 0.068-0.616) and 0.022% (IQR 0.008-0.082) of the malaria-attributable erythrocyte loss in participants inoculated with Pf3D7, PfK13, and P. vivax, respectively.
Conclusion: Early experimental P. falciparum and P. vivax infection resulted in a small but significant fall in haemoglobin despite parasitaemia only just at the level of microscopic detection. Loss of parasitized erythrocytes accounted for < 0.2% of the total malaria-attributable haemoglobin loss.
Keywords: Anaemia; CHMI; Induced blood-stage malaria; Malaria; Plasmodium falciparum; VIS.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Loss of complement regulatory proteins on red blood cells in mild malarial anaemia and in Plasmodium falciparum induced blood-stage infection.Malar J. 2019 Sep 18;18(1):312. doi: 10.1186/s12936-019-2962-0. Malar J. 2019. PMID: 31533836 Free PMC article.
-
The risk of Plasmodium vivax parasitaemia after P. falciparum malaria: An individual patient data meta-analysis from the WorldWide Antimalarial Resistance Network.PLoS Med. 2020 Nov 19;17(11):e1003393. doi: 10.1371/journal.pmed.1003393. eCollection 2020 Nov. PLoS Med. 2020. PMID: 33211712 Free PMC article.
-
Risk of Plasmodium vivax parasitaemia after Plasmodium falciparum infection: a systematic review and meta-analysis.Lancet Infect Dis. 2019 Jan;19(1):91-101. doi: 10.1016/S1473-3099(18)30596-6. Lancet Infect Dis. 2019. PMID: 30587297 Free PMC article.
-
Active case detection, treatment of falciparum malaria with combined chloroquine and sulphadoxine/pyrimethamine and vivax malaria with chloroquine and molecular markers of anti-malarial resistance in the Republic of Vanuatu.Malar J. 2010 Apr 6;9:89. doi: 10.1186/1475-2875-9-89. Malar J. 2010. PMID: 20370920 Free PMC article.
-
Prevalence and risk factors related to poor outcome of patients with severe Plasmodium vivax infection: a systematic review, meta-analysis, and analysis of case reports.BMC Infect Dis. 2020 May 24;20(1):363. doi: 10.1186/s12879-020-05046-y. BMC Infect Dis. 2020. PMID: 32448216 Free PMC article.
Cited by
-
Characterizing the Blood-Stage Antimalarial Activity of Tafenoquine in Healthy Volunteers Experimentally Infected With Plasmodium falciparum.Clin Infect Dis. 2023 Jun 8;76(11):1919-1927. doi: 10.1093/cid/ciad075. Clin Infect Dis. 2023. PMID: 36795050 Free PMC article.
-
Sterile protection against P. vivax malaria by repeated blood stage infection in the Aotus monkey model.Life Sci Alliance. 2023 Dec 29;7(3):e202302524. doi: 10.26508/lsa.202302524. Print 2024 Mar. Life Sci Alliance. 2023. PMID: 38158220 Free PMC article.
-
Epidemiological characteristics of P. vivax asymptomatic infections in the Peruvian Amazon.Front Cell Infect Microbiol. 2022 Aug 31;12:901423. doi: 10.3389/fcimb.2022.901423. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36118037 Free PMC article.
-
Systems biology of malaria explored with nonhuman primates.Malar J. 2022 Jun 7;21(1):177. doi: 10.1186/s12936-022-04199-2. Malar J. 2022. PMID: 35672852 Free PMC article. Review.
References
-
- WHO . World Malaria Report 2020. Geneva: World Health Organization; 2020.
-
- WHO . The potential impact of health service disruptions on the burden of malaria 2020. Geneva: World Health Organization; 2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
