

X-linked sideroblastic anaemia in a female fetus: a case report and a literature review
- PMID: 34930268
- PMCID: PMC8686580
- DOI: 10.1186/s12920-021-01146-z
X-linked sideroblastic anaemia in a female fetus: a case report and a literature review
Abstract
Background: X-linked sideroblastic anaemia (XLSA) is commonly due to mutations in the ALAS2 gene and predominantly affects hemizygous males. Heterozygous female carriers of the ALAS2 gene mutation are often asymptomatic or only mildly anaemic. XLSA is usually characterized by microcytic erythrocytes (reduced mean corpuscular volume (MCV)) and hypochromia, along with increased red cell distribution width. However, in females with XLSA the characteristic laboratory findings can be dimorphic and present with macrocytic (elevated MCV) in addition to microcytic red cells.
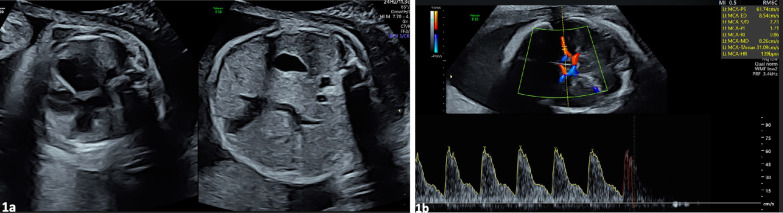
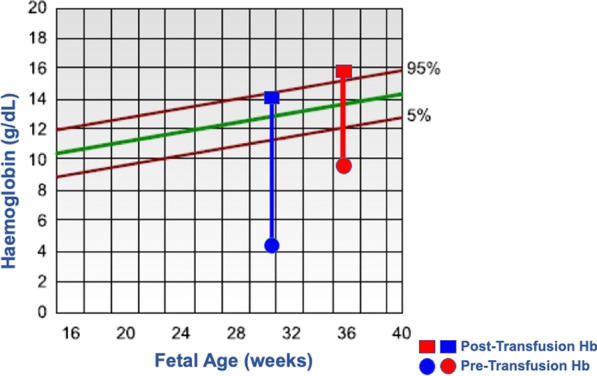
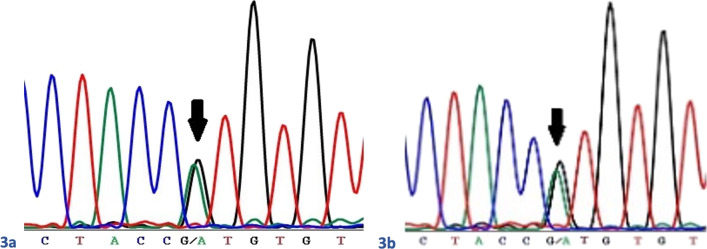
Case presentation: We report a case of fetal anaemia, presenting in the early third trimester of pregnancy, in a female fetus. Ultrasound findings at 29 weeks were of cardiomegaly, prominent umbilical veins, a small rim of ascites, and mean cerebral artery peak systolic velocity (PSV) value above 1.5 Multiples of the Median (MoM). She underwent non-invasive prenatal testing that determined the rhesus genotype of the fetus to be rhesus B negative. No red blood cell antibodies were reported. Other investigations to determine the underlying cause of fetal anaemia included microarray comparative genomic hybridization, serology to exclude congenital infection and a peripheral blood film and fetal bilirubin to detect haemolysis. The maternal grandmother had a history of sideroblastic anaemia diagnosed at the age of 17 years. The mother had mild macrocytic anaemia with haemoglobin of 10.4 g/dl and MCV of 104 fl. The fetal anaemia was successfully treated with two in utero transfusions (IUTs), and delivery occurred via caesarean section at 37 weeks of gestation. The red cell gene sequencing in both the mother and fetus were heterozygous for an ALAS2 mutation causing in utero manifestations of XLSA. The haemoglobin on discharge to the local hospital at five days of age was 19.1 g/dl. Subsequently, the infant became anaemic, requiring regular 3-4 monthly blood transfusions and demonstrating overall normal development. Her anaemia was unresponsive to pyridoxine.
Conclusions: This is one of four cases reporting multiple female members presenting with discordant clinical features of XLSA from being entirely asymptomatic to hydropic in utero. Our report is novel in that there are no previous cases in the literature of anaemia in a female fetus heterozygous for ALAS2 mutation.
Keywords: ALAS2 mutation; Sideroblastic anaemia; X-linked.
© 2021. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
The role of genetic testing in accurate diagnosis of X-linked sideroblastic anemia: novel ALAS2 mutations and the impact of X-chromosome inactivation.Sci Rep. 2025 Apr 7;15(1):11843. doi: 10.1038/s41598-025-95590-x. Sci Rep. 2025. PMID: 40195342 Free PMC article.
-
Absent phenotypic expression of X-linked sideroblastic anemia in one of 2 brothers with a novel ALAS2 mutation.Blood. 2002 Dec 1;100(12):4236-8. doi: 10.1182/blood-2002-03-0685. Epub 2002 Aug 8. Blood. 2002. PMID: 12393718
-
A hemizygous p.R204Q mutation in the ALAS2 gene underlies X-linked sideroblastic anemia in an adult Chinese Han man.BMC Med Genomics. 2021 Apr 15;14(1):107. doi: 10.1186/s12920-021-00950-x. BMC Med Genomics. 2021. PMID: 33858445 Free PMC article.
-
[Congenital sideroblastic anemia-a new family with identification of K156E mutation of ALAS2 gene and literature review].Zhonghua Xue Ye Xue Za Zhi. 2014 Feb;35(2):142-6. doi: 10.3760/cma.j.issn.0253-2727.2014.02.018. Zhonghua Xue Ye Xue Za Zhi. 2014. PMID: 24606657 Review. Chinese.
-
Pyridoxine-refractory congenital sideroblastic anaemia with evidence for autosomal inheritance: exclusion of linkage to ALAS2 at Xp11.21 by polymorphism analysis.J Med Genet. 1994 Mar;31(3):213-8. doi: 10.1136/jmg.31.3.213. J Med Genet. 1994. PMID: 7912287 Free PMC article. Review.
Cited by
-
The role of genetic testing in accurate diagnosis of X-linked sideroblastic anemia: novel ALAS2 mutations and the impact of X-chromosome inactivation.Sci Rep. 2025 Apr 7;15(1):11843. doi: 10.1038/s41598-025-95590-x. Sci Rep. 2025. PMID: 40195342 Free PMC article.
-
Multidisciplinary approaches to study anaemia with special mention on aplastic anaemia (Review).Int J Mol Med. 2024 Nov;54(5):95. doi: 10.3892/ijmm.2024.5419. Epub 2024 Sep 2. Int J Mol Med. 2024. PMID: 39219286 Free PMC article. Review.
-
Slc6a20a Heterozygous and Homozygous Mutant Mice Display Differential Behavioral and Transcriptomic Changes.Front Mol Neurosci. 2022 Mar 7;15:857820. doi: 10.3389/fnmol.2022.857820. eCollection 2022. Front Mol Neurosci. 2022. PMID: 35321029 Free PMC article.
-
A novel and apparent de novo ALAS2 missense variant associated with congenital sideroblastic anemia.Front Pediatr. 2024 Aug 29;12:1411676. doi: 10.3389/fped.2024.1411676. eCollection 2024. Front Pediatr. 2024. PMID: 39281190 Free PMC article.
-
Three-generation female cohort with macrocytic anemia and iron overload.Am J Hematol. 2025 Jan;100(1):133-138. doi: 10.1002/ajh.27489. Epub 2024 Sep 27. Am J Hematol. 2025. PMID: 39329459 Free PMC article. No abstract available.
References
-
- Bergmann AK, Campagna DR, McLoughlin EM, Agarwal S, Fleming MD, Bottomley SS, et al. Systematic molecular genetic analysis of congenital sideroblastic anemia: evidence for genetic heterogeneity and identification of novel mutations. Pediatr Blood Cancer. 2010;54:273–278. doi: 10.1002/pbc.22244. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
