

Impact of COVID-19 on routine malaria indicators in rural Uganda: an interrupted time series analysis
- PMID: 34930317
- PMCID: PMC8685800
- DOI: 10.1186/s12936-021-04018-0
Impact of COVID-19 on routine malaria indicators in rural Uganda: an interrupted time series analysis
Abstract
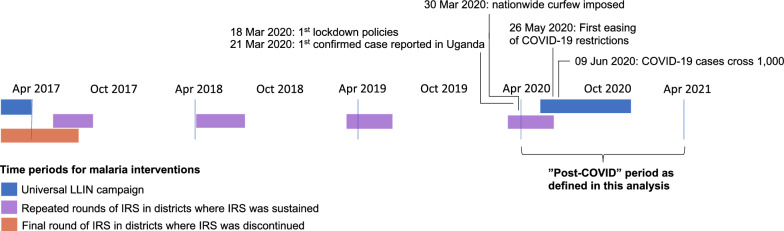
Background: In March 2020, the government of Uganda implemented a strict lockdown policy in response to the COVID-19 pandemic. Interrupted time series analysis (ITSA) was performed to assess whether major changes in outpatient attendance, malaria burden, and case management occurred after the onset of the COVID-19 epidemic in rural Uganda.
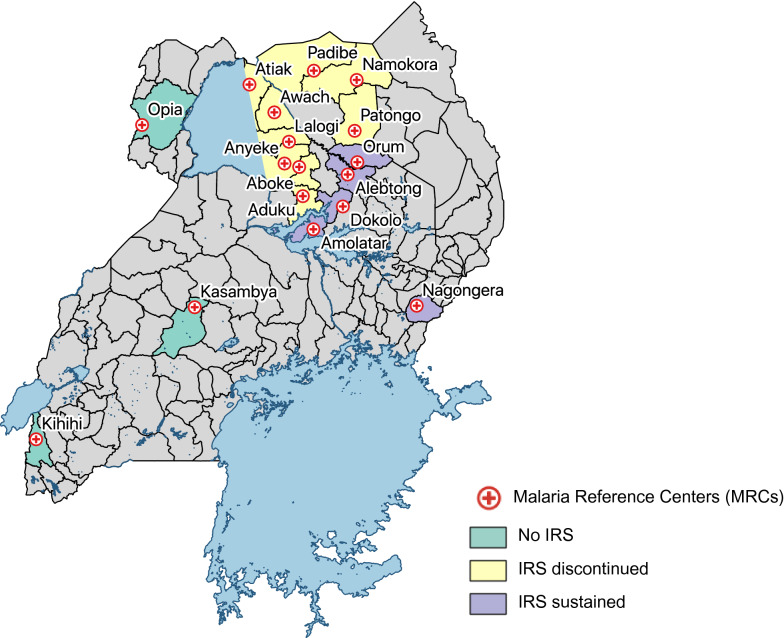
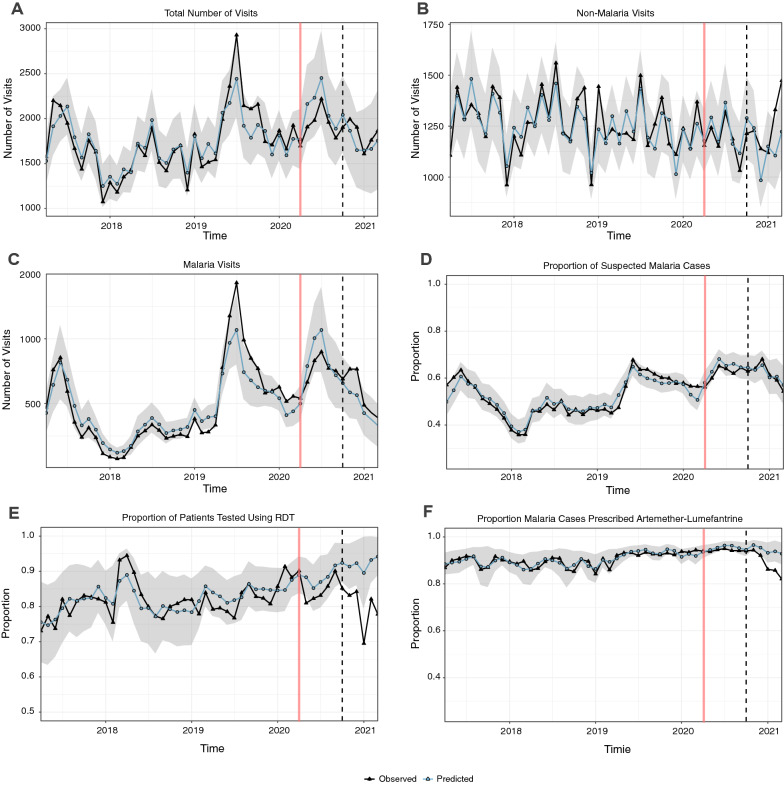
Methods: Individual level data from all outpatient visits collected from April 2017 to March 2021 at 17 facilities were analysed. Outcomes included total outpatient visits, malaria cases, non-malarial visits, proportion of patients with suspected malaria, proportion of patients tested using rapid diagnostic tests (RDTs), and proportion of malaria cases prescribed artemether-lumefantrine (AL). Poisson regression with generalized estimating equations and fractional regression was used to model count and proportion outcomes, respectively. Pre-COVID trends (April 2017-March 2020) were used to predict the'expected' trend in the absence of COVID-19 introduction. Effects of COVID-19 were estimated over two six-month COVID-19 time periods (April 2020-September 2020 and October 2020-March 2021) by dividing observed values by expected values, and expressed as ratios.
Results: A total of 1,442,737 outpatient visits were recorded. Malaria was suspected in 55.3% of visits and 98.8% of these had a malaria diagnostic test performed. ITSA showed no differences between observed and expected total outpatient visits, malaria cases, non-malarial visits, or proportion of visits with suspected malaria after COVID-19 onset. However, in the second six months of the COVID-19 time period, there was a smaller mean proportion of patients tested with RDTs compared to expected (relative prevalence ratio (RPR) = 0.87, CI (0.78-0.97)) and a smaller mean proportion of malaria cases prescribed AL (RPR = 0.94, CI (0.90-0.99)).
Conclusions: In the first year after the COVID-19 pandemic arrived in Uganda, there were no major effects on malaria disease burden and indicators of case management at these 17 rural health facilities, except for a modest decrease in the proportion of RDTs used for malaria diagnosis and the mean proportion of malaria cases prescribed AL in the second half of the COVID-19 pandemic year. Continued surveillance will be essential to monitor for changes in trends in malaria indicators so that Uganda can quickly and flexibly respond to challenges imposed by COVID-19.
© 2021. The Author(s).
Conflict of interest statement
None to declare.
Figures
Update of
-
Impact of COVID-19 on routine malaria indicators in Uganda: An interrupted time series analysis.Res Sq [Preprint]. 2021 Aug 18:rs.3.rs-819495. doi: 10.21203/rs.3.rs-819495/v1. Res Sq. 2021. Update in: Malar J. 2021 Dec 20;20(1):475. doi: 10.1186/s12936-021-04018-0. PMID: 34426808 Free PMC article. Updated. Preprint.
References
-
- WHO. World Malaria Report 2020. Geneva, World Health Organization, 2020. Accessed from: https://www.who.int/publications/i/item/9789240015791 on 19 April 2021. 2020.
-
- Weiss DJ, Bertozzi-Villa A, Rumisha SF, Amratia P, Arambepola R, Battle KE, et al. Indirect effects of the COVID-19 pandemic on malaria intervention coverage, morbidity, and mortality in Africa: a geospatial modelling analysis. Lancet Infect Dis. 2021;21:59–69. doi: 10.1016/S1473-3099(20)30700-3. - DOI - PMC - PubMed
-
- Hogan AB, Jewell BL, Sherrard-Smith E, Vesga JF, Watson OJ, Whittaker C, et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: a modelling study. Lancet Glob Health. 2020;8:e1132–e1141. doi: 10.1016/S2214-109X(20)30288-6. - DOI - PMC - PubMed
-
- Ministry of Health. Overview of Malaria in Uganda (2014 – 2020). Accessed from: https://www.health.go.ug/programs/national-malaria-control-program/#:~:t... on 29 July 2021.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
