

Bench test and in vivo evaluation of longitudinal stent deformation during proximal optimisation
- PMID: 34930716
- PMCID: PMC9904376
- DOI: 10.4244/EIJ-D-21-00824
Bench test and in vivo evaluation of longitudinal stent deformation during proximal optimisation
Abstract
Background: While radial stent deformation has been thoroughly investigated, data on longitudinal deformation are scarce.
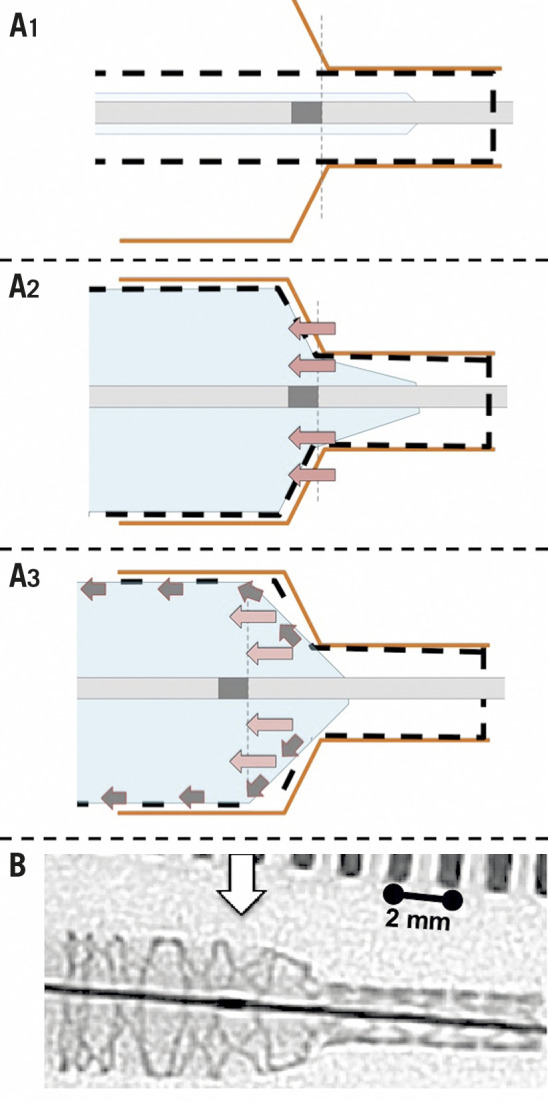
Aims: The aim of the study was to describe longitudinal stent deformation associated with the proximal optimisation technique (POT).
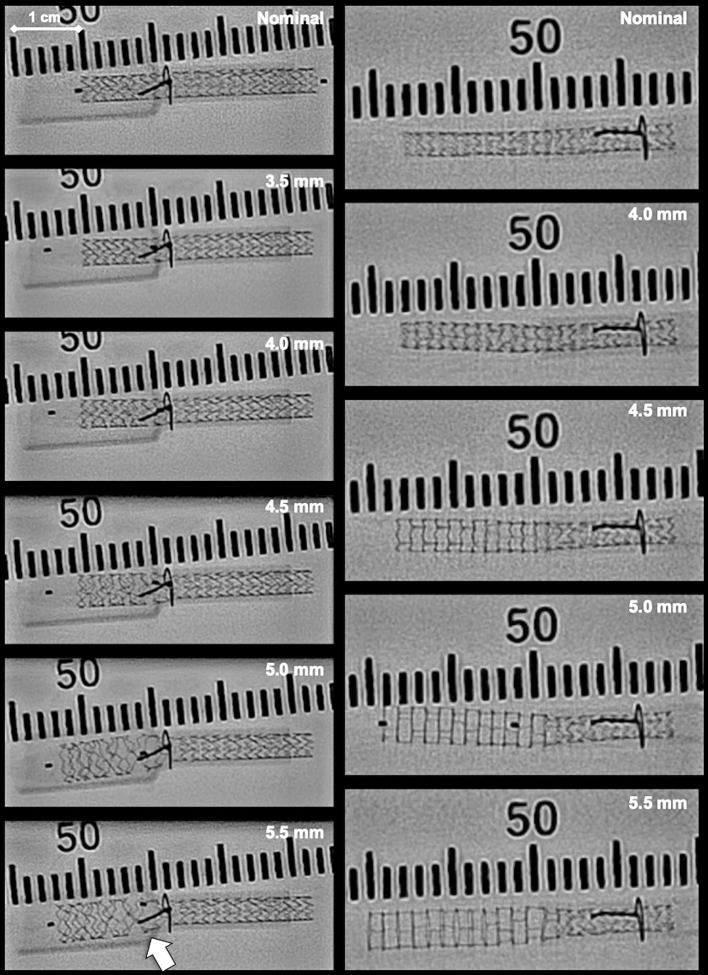
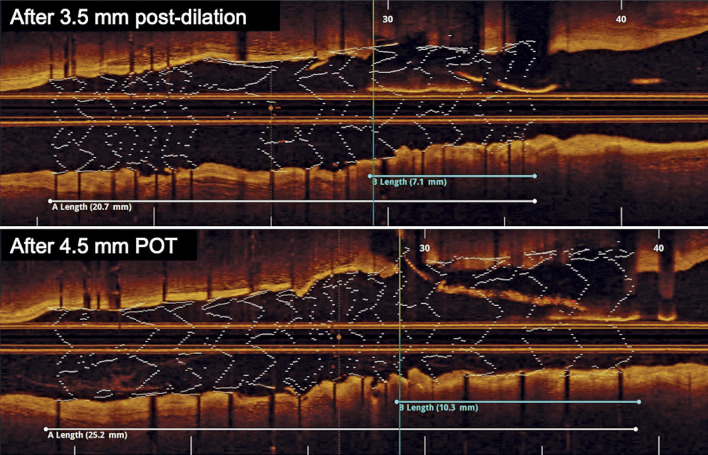
Methods: Longitudinal stent deformation was assessed by bench testing and by clinical evaluation. Bench testing was performed in silicone models using 3.00 (n=15) and 3.50 mm (n=14) stent platforms. After deployment, stents were sequentially post-dilated in the proximal main branch up to 5.50 mm, in increments of 0.50 mm, in order to simulate a spectrum of overexpansion. Stent length was redefined by optical coherence tomography (OCT) after each step. Clinical data were collected retrospectively from OCT-guided bifurcation percutaneous coronary intervention cases.
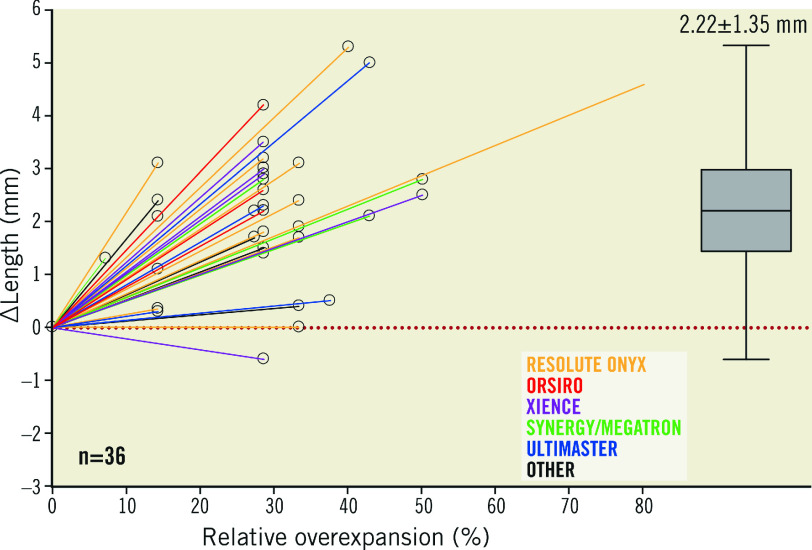
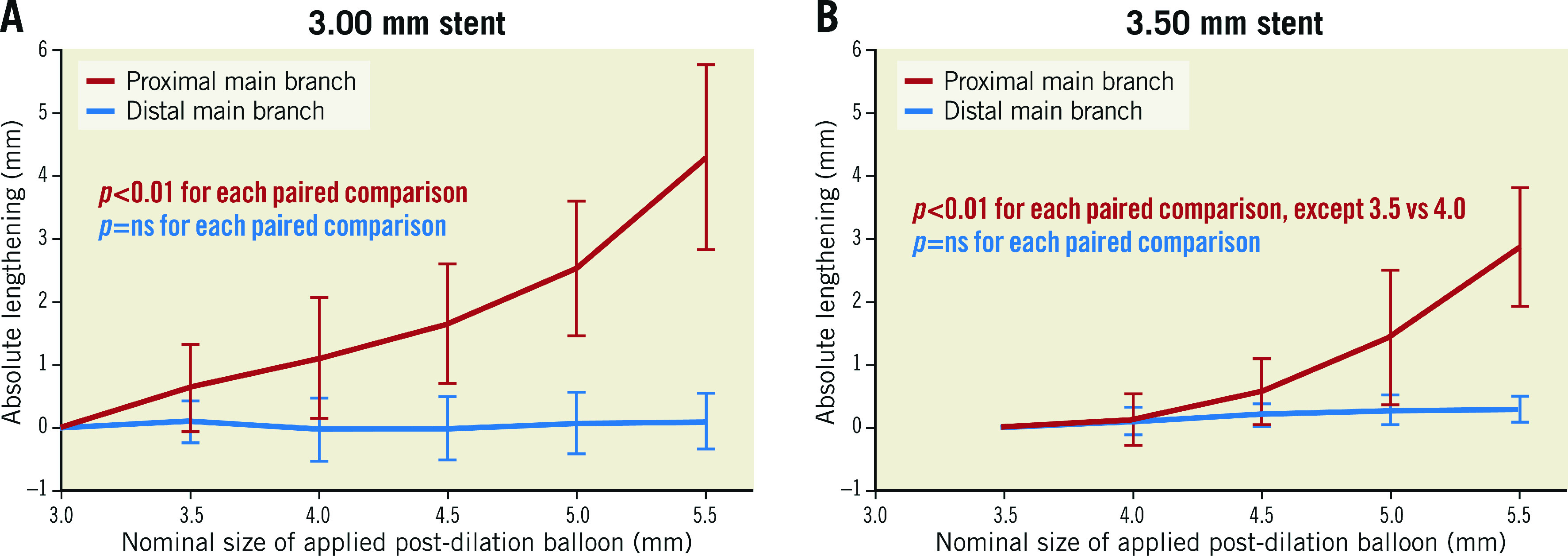
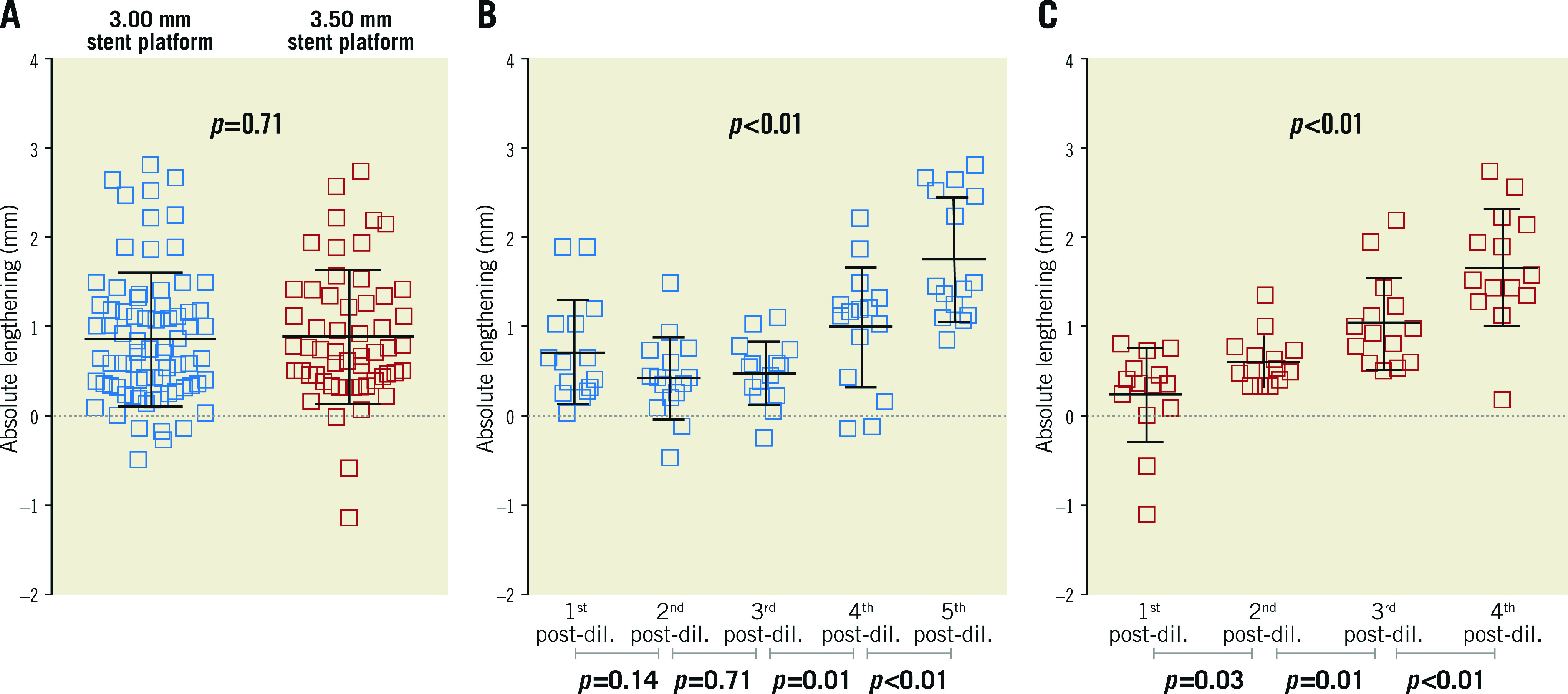
Results: In bench tests, POT has led to significant stent elongation in all cases. The magnitude of elongation was comparable between the 3.00 and the 3.50 mm stent platforms, with 0.86±0.74 mm vs 0.86±0.73 mm, respectively (p=0.71), per 0.5 mm overexpansion. For 3.00 mm stent platforms, maximal elongation was 4.31±1.47 mm after up to 5.5 mm overexpansion. For 3.50 mm platforms, maximal elongation was 2.87±0.94 mm after up to 5.5 mm overexpansion. Thirty-six clinical cases were analysed, of which 22 (61%) were performed in the distal left main. Post-dilation was performed with 0.98±0.36 mm absolute overexpansion, resulting in 2.22±1.35 mm elongation, as compared to nominal stent length.
Conclusions: Overexpansion by POT results in proximal stent elongation. This has to be considered once the stent length is selected and the stent is positioned, especially in the left main stem, where proximal overexpansion is marked and accurate ostial landing is critical.
Conflict of interest statement
G. Toth receives personal fees from Abbott, Medtronic, Terumo and Biotronik, outside the present work. T. Johnson has received personal fees from Abbott, Boston Scientific, Medtronic and Terumo, outside the present work. W. Wijns has received institutional research grants from MicroPort and is supported by a Science Foundation Ireland Research Professorship grant (15/RP/2765). X. Wu, M. Lunardi and A. Shahzad are supported by a Science Foundation Ireland Research Professorship grant (15/RP/2765). The other authors have no conflicts of interest to declare.
Figures
References
-
- Burzotta F, Lassen JF, Lefèvre T, Banning AP, Chatzizisis YS, Johnson TW, Ferenc M, Rathore S, Albiero R, Pan M, Darremont O, Hildick-Smith D, Chieffo A, Zimarino M, Louvard Y, Stankovic G. Percutaneous coronary intervention for bifurcation coronary lesions: the 15th consensus document from the European Bifurcation Club. EuroIntervention. 2021;16:1307–17. - PMC - PubMed
-
- Finet G, Derimay F, Motreff P, Guerin P, Pilet P, Ohayon J, Darremont O, Rioufol G. Comparative Analysis of Sequential Proximal Optimizing Technique Versus Kissing Balloon Inflation Technique in Provisional Bifurcation Stenting: Fractal Coronary Bifurcation Bench Test. JACC Cardiovasc Interv. 2015;8:1308–17. - PubMed
-
- Kassab GS, Finet G. Anatomy and function relation in the coronary tree: from bifurcations to myocardial flow and mass. EuroIntervention. 2015;11 Suppl V:V13–7. - PubMed
-
- Finet G, Gilard M, Perrenot B, Rioufol G, Motreff P, Gavit L, Prost R. Fractal geometry of arterial coronary bifurcations: a quantitative coronary angiography and intravascular ultrasound analysis. EuroIntervention. 2008;3:490–8. - PubMed
-
- Foin N, Sen S, Allegria E, Petraco R, Nijjer S, Francis DP, Di Mario, Davies JE. Maximal expansion capacity with current DES platforms: a critical factor for stent selection in the treatment of left main bifurcations? EuroIntervention. 2013;8:1315–25. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources