

Smartphone-based digital phenotyping for dry eye toward P4 medicine: a crowdsourced cross-sectional study
- PMID: 34931013
- PMCID: PMC8688467
- DOI: 10.1038/s41746-021-00540-2
Smartphone-based digital phenotyping for dry eye toward P4 medicine: a crowdsourced cross-sectional study
Abstract
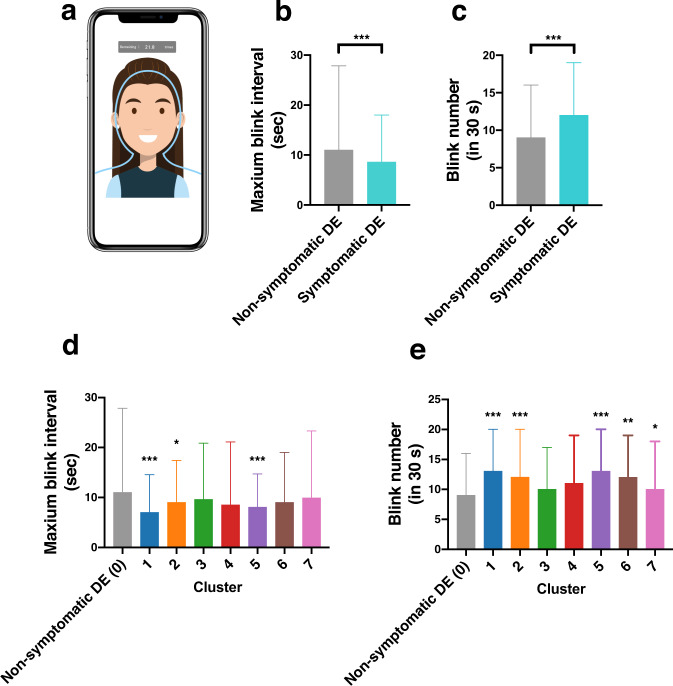
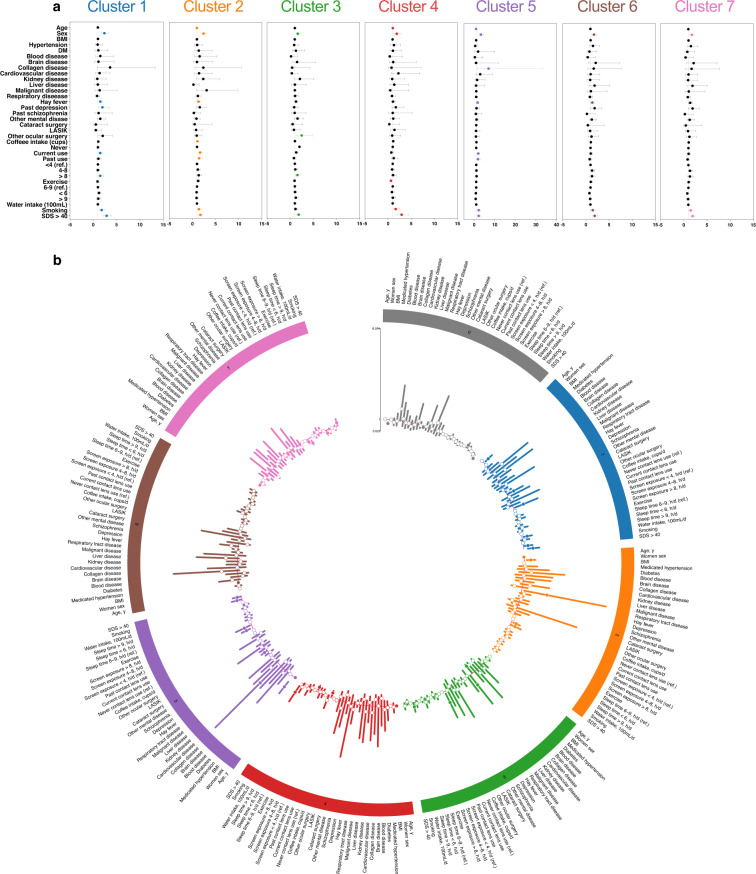
Multidimensional integrative data analysis of digital phenotyping is crucial for elucidating the pathologies of multifactorial and heterogeneous diseases, such as the dry eye (DE). This crowdsourced cross-sectional study explored a novel smartphone-based digital phenotyping strategy to stratify and visualize the heterogenous DE symptoms into distinct subgroups. Multidimensional integrative data were collected from 3,593 participants between November 2016 and September 2019. Dimension reduction via Uniform Manifold Approximation and Projection stratified the collected data into seven clusters of symptomatic DE. Symptom profiles and risk factors in each cluster were identified by hierarchical heatmaps and multivariate logistic regressions. Stratified DE subgroups were visualized by chord diagrams, co-occurrence networks, and Circos plot analyses to improve interpretability. Maximum blink interval was reduced in clusters 1, 2, and 5 compared to non-symptomatic DE. Clusters 1 and 5 had severe DE symptoms. A data-driven multidimensional analysis with digital phenotyping may establish predictive, preventive, personalized, and participatory medicine.
© 2021. The Author(s).
Conflict of interest statement
The DryEyeRhythm app was created using Apple’s ResearchKit (Cupertino, CA, USA) along with OHAKO, Inc. (Tokyo, Japan) and Medical Logue, Inc. (Tokyo, Japan). Y.O. and T.I. are the owners of InnoJin, Inc., Tokyo, Japan for developing DryEyeRhytm. T.I. reported receiving grants from Johnson & Johnson Vision Care, SEED Co., Ltd, Novartis Pharma K.K., and Kowa Company, Ltd. outside the submitted work, as well as personal fees from Santen Pharmaceutical Co., Ltd., and InnoJin, Inc. A.M. reported receiving grants from Johnson & Johnson Vision Care and Santen Pharmaceutical Co., Ltd. The remaining authors declare no competing interests.
Figures




References
-
- Craig JP, et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017;15:276–283. - PubMed
-
- Tsubota K, et al. New Perspectives on Dry Eye Definition and Diagnosis: A Consensus Report by the Asia Dry Eye Society. Ocul. Surf. 2017;15:65–76. - PubMed
-
- Kaido M, Ishida R, Dogru M, Tsubota K. The relation of functional visual acuity measurement methodology to tear functions and ocular surface status. Jpn J. Ophthalmol. 2011;55:451–459. - PubMed
LinkOut - more resources
Full Text Sources
