

Association of Rivaroxaban vs Apixaban With Major Ischemic or Hemorrhagic Events in Patients With Atrial Fibrillation
- PMID: 34932078
- PMCID: PMC8693217
- DOI: 10.1001/jama.2021.21222
Association of Rivaroxaban vs Apixaban With Major Ischemic or Hemorrhagic Events in Patients With Atrial Fibrillation
Erratum in
-
Error in Figure.JAMA. 2022 Apr 5;327(13):1294. doi: 10.1001/jama.2022.4059. JAMA. 2022. PMID: 35380601 Free PMC article. No abstract available.
Abstract
Importance: The comparative effectiveness of rivaroxaban and apixaban, the most frequently prescribed oral anticoagulants for ischemic stroke prevention in patients with atrial fibrillation, is uncertain.
Objective: To compare major ischemic and hemorrhagic outcomes in patients with atrial fibrillation treated with rivaroxaban or apixaban.
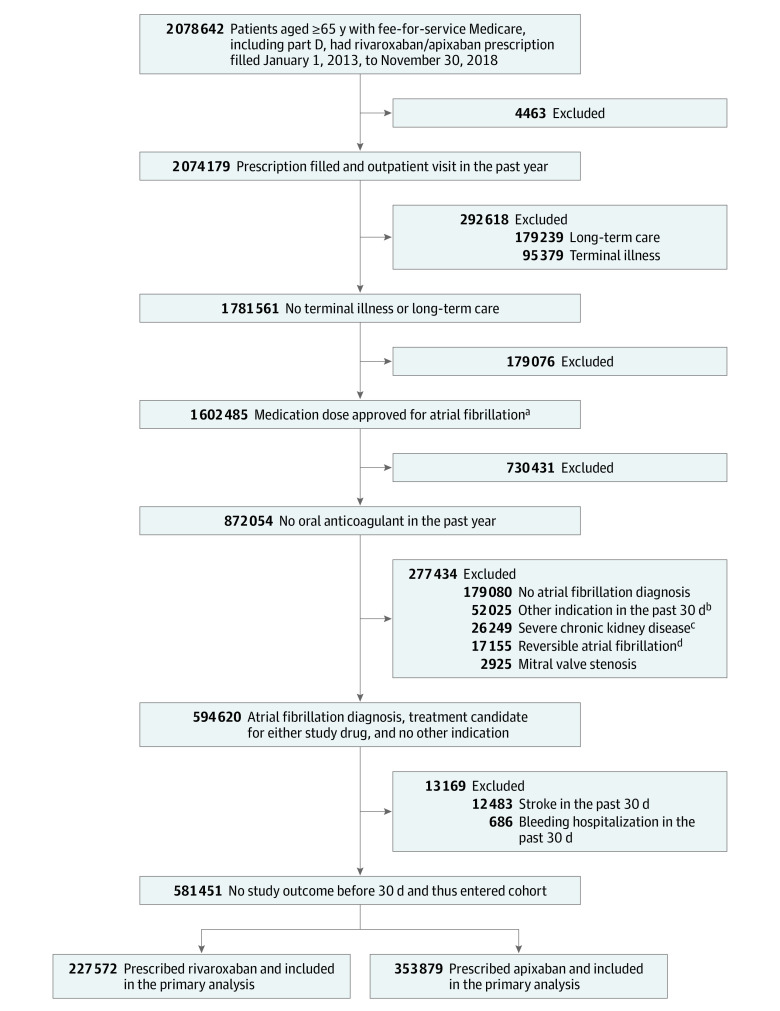
Design, setting, and participants: Retrospective cohort study using computerized enrollment and claims files for US Medicare beneficiaries 65 years or older. Between January 1, 2013, and November 30, 2018, a total of 581 451 patients with atrial fibrillation began rivaroxaban or apixaban treatment and were followed up for 4 years, through November 30, 2018.
Exposures: Rivaroxaban (n = 227 572) and apixaban (n = 353 879), either standard or reduced dose.
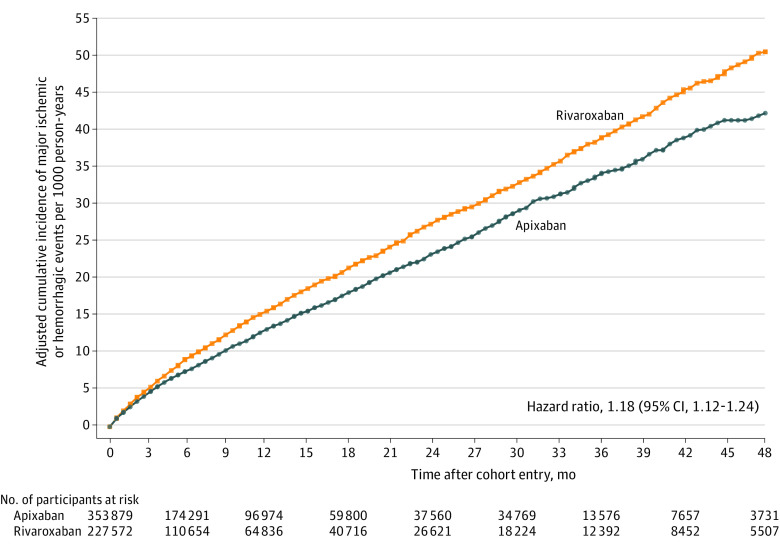
Main outcomes and measures: The primary outcome was a composite of major ischemic (stroke/systemic embolism) and hemorrhagic (intracerebral hemorrhage/other intracranial bleeding/fatal extracranial bleeding) events. Secondary outcomes were nonfatal extracranial bleeding and total mortality (fatal ischemic/hemorrhagic event or other death during follow-up). Rates, hazard ratios (HRs), and rate differences (RDs) were adjusted for baseline differences in comorbidity with inverse probability of treatment weighting.
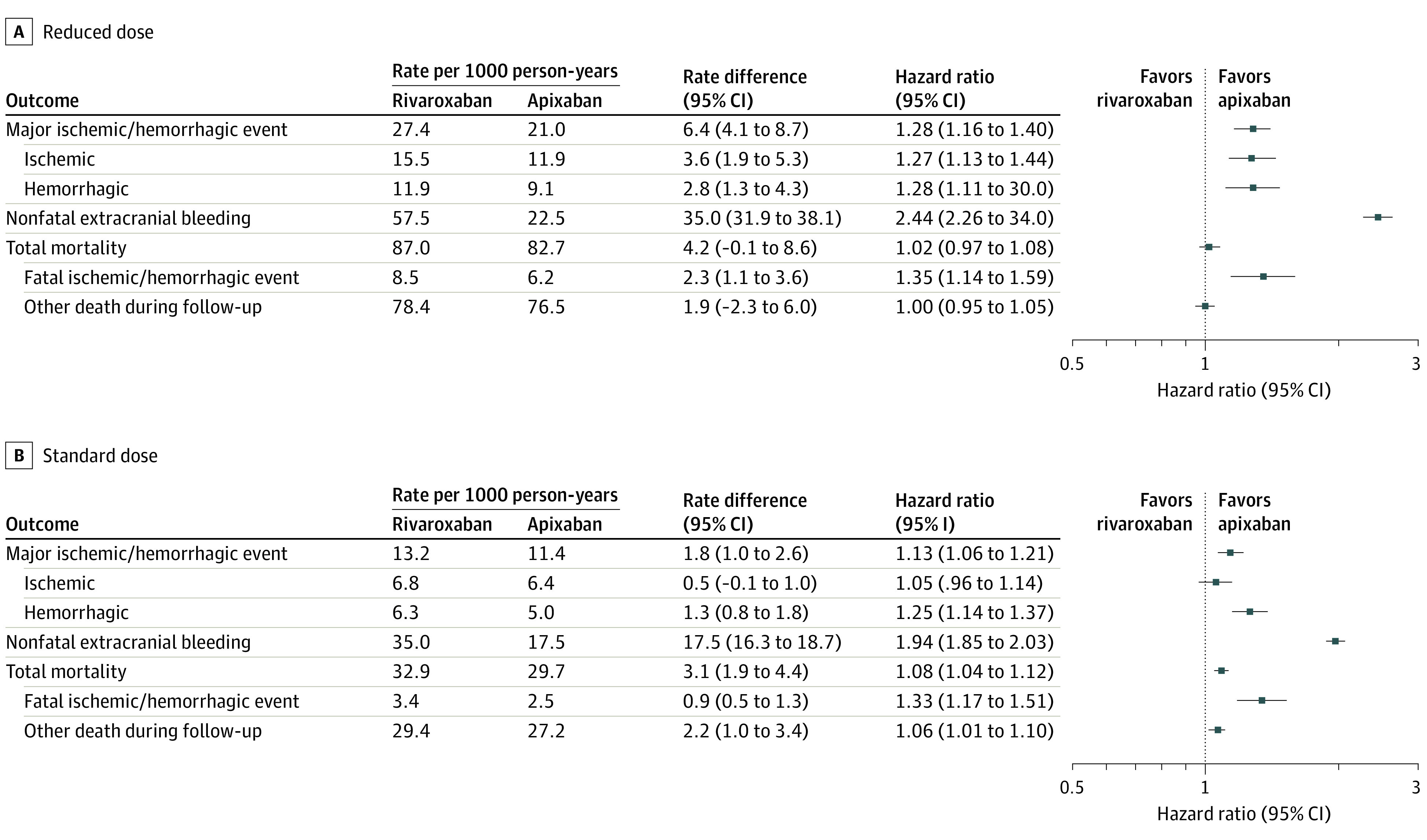
Results: Study patients (mean age, 77.0 years; 291 966 [50.2%] women; 134 393 [23.1%] receiving reduced dose) had 474 605 person-years of follow-up (median [IQR] of 174 [62-397] days). The adjusted primary outcome rate for rivaroxaban was 16.1 per 1000 person-years vs 13.4 per 1000 person-years for apixaban (RD, 2.7 [95% CI, 1.9-3.5]; HR, 1.18 [95% CI, 1.12-1.24]). The rivaroxaban group had increased risk for both major ischemic events (8.6 vs 7.6 per 1000 person-years; RD, 1.1 [95% CI, 0.5-1.7]; HR, 1.12 [95% CI, 1.04-1.20]) and hemorrhagic events (7.5 vs 5.9 per 1000 person-years; RD, 1.6 [95% CI, 1.1-2.1]; HR, 1.26 [95% CI, 1.16-1.36]), including fatal extracranial bleeding (1.4 vs 1.0 per 1000 person-years; RD, 0.4 [95% CI, 0.2-0.7]; HR, 1.41 [95% CI, 1.18-1.70]). Patients receiving rivaroxaban had increased risk of nonfatal extracranial bleeding (39.7 vs 18.5 per 1000 person-years; RD, 21.1 [95% CI, 20.0-22.3]; HR, 2.07 [95% CI, 1.99-2.15]), fatal ischemic/hemorrhagic events (4.5 vs 3.3 per 1000 person-years; RD, 1.2 [95% CI, 0.8-1.6]; HR, 1.34 [95% CI, 1.21-1.48]), and total mortality (44.2 vs 41.0 per 1000 person-years; RD, 3.1 [95% CI, 1.8-4.5]; HR, 1.06 [95% CI, 1.02-1.09]). The risk of the primary outcome was increased for rivaroxaban in both those receiving the reduced dose (27.4 vs 21.0 per 1000 person-years; RD, 6.4 [95% CI, 4.1-8.7]; HR, 1.28 [95% CI, 1.16-1.40]) and the standard dose (13.2 vs 11.4 per 1000 person-years; RD, 1.8 [95% CI, 1.0-2.6]; HR, 1.13 [95% CI, 1.06-1.21]) groups.
Conclusions and relevance: Among Medicare beneficiaries 65 years or older with atrial fibrillation, treatment with rivaroxaban compared with apixaban was associated with a significantly increased risk of major ischemic or hemorrhagic events.
Conflict of interest statement
Figures
Comment in
-
Informing the Choice of Direct Oral Anticoagulant Therapy in Patients With Atrial Fibrillation.JAMA. 2021 Dec 21;326(23):2372-2374. doi: 10.1001/jama.2021.21305. JAMA. 2021. PMID: 34932097 No abstract available.
-
Rivaroxaban vs Apixaban and Ischemic or Hemorrhagic Events in Patients With Atrial Fibrillation.JAMA. 2022 Apr 5;327(13):1290. doi: 10.1001/jama.2022.1425. JAMA. 2022. PMID: 35380590 No abstract available.
References
-
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125-e151. doi: 10.1161/CIR.0000000000000665 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
