

Dual PD-1 and CTLA-4 Checkpoint Blockade Using Balstilimab and Zalifrelimab Combination as Second-Line Treatment for Advanced Cervical Cancer: An Open-Label Phase II Study
- PMID: 34932394
- PMCID: PMC8887945
- DOI: 10.1200/JCO.21.02067
Dual PD-1 and CTLA-4 Checkpoint Blockade Using Balstilimab and Zalifrelimab Combination as Second-Line Treatment for Advanced Cervical Cancer: An Open-Label Phase II Study
Abstract
Purpose: Balstilimab (antiprogrammed death-1) and zalifrelimab (anticytotoxic T-lymphocyte-associated antigen-4) are two new checkpoint inhibitors emerging as promising investigational agents for the treatment of advanced cervical cancer. This phase II trial (ClinicalTrials.gov identifier: NCT03495882) evaluated the combination of balstilimab plus zalifrelimab in patients with recurrent and/or metastatic cervical cancer who relapsed after prior platinum-based therapy.
Patients and methods: Patients were intravenously dosed with balstilimab 3 mg/kg once every 2 weeks and zalifrelimab 1 mg/kg once every 6 weeks, for up to 24 months. The primary end point was objective response rate (ORR, RECIST version 1.1, assessed by independent central review). Secondary end points included duration of response, safety and tolerability, and survival.
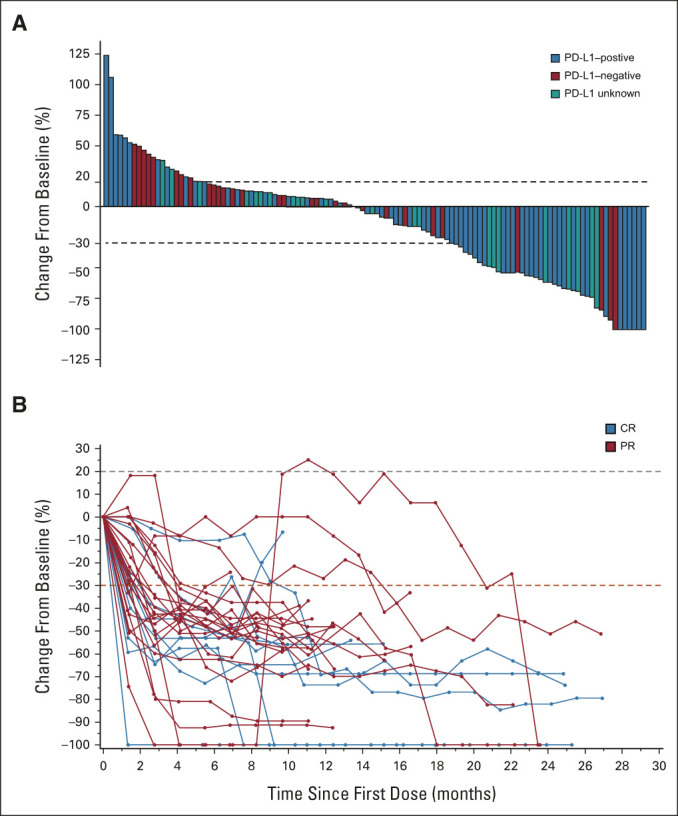
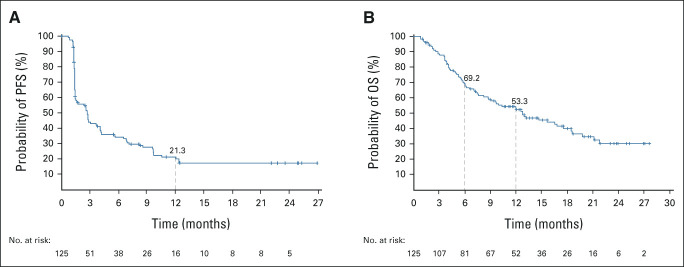
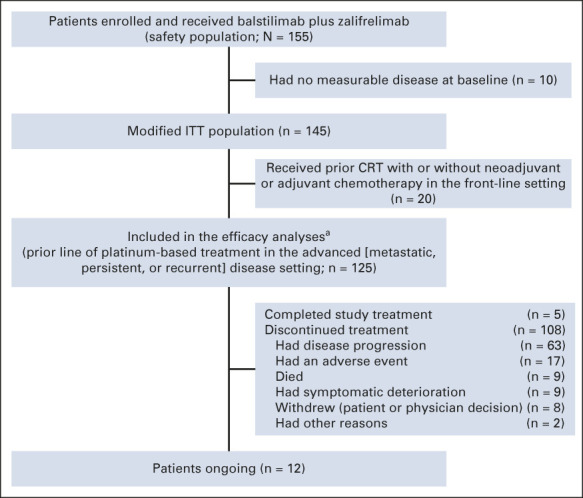
Results: In total, 155 women (median age, 50 years [range, 24-76 years]) were enrolled and treated with balstilimab plus zalifrelimab; 125 patients had measurable disease at baseline and one prior line of platinum-based therapy in the advanced setting, and these patients constituted the efficacy-evaluable population. The median follow-up was 21 months. The confirmed ORR was 25.6% (95% CI, 18.8 to 33.9), including 10 complete responders and 22 partial responders, with median duration of response not reached (86.5%, 75.5%, and 64.2% at 6, 9, and 12 months, respectively). The ORRs were 32.8% and 9.1% in patients with programmed death ligand-1-positive and programmed death ligand-1-negative tumors, respectively. For patients with squamous cell carcinoma, the ORR was 32.6%. The overall disease control rate was 52% (95% CI, 43.3 to 60.6). Hypothyroidism (14.2%) and hyperthyroidism (7.1%) were the most common immune-mediated adverse events.
Conclusion: Promising and durable clinical activity, with favorable tolerability, was seen in this largest trial to date evaluating dual programmed death-1/cytotoxic T-lymphocyte-associated antigen-4 blockade in patients with recurrent and/or metastatic cervical cancer. Further investigation of the balstilimab and zalifrelimab combination in this setting is continuing.
Conflict of interest statement
Figures
Comment in
-
Abscobal Effect of Balstilimab and Zalifrelimab Combination as Second-Line Treatment for Advanced Cervical Cancer.J Clin Oncol. 2022 Jul 1;40(19):2177-2178. doi: 10.1200/JCO.22.00084. Epub 2022 Apr 29. J Clin Oncol. 2022. PMID: 35486885 No abstract available.
References
-
- Boussios S, Seraj E, Zarkavelis G, et al. : Management of patients with recurrent/advanced cervical cancer beyond first line platinum regimens: Where do we stand? A literature review. Crit Rev Oncol Hematol 108:164-174, 2016 - PubMed
-
- Marth C, Landoni F, Mahner S, et al. : Cervical cancer: ESMO clinical Practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 28:iv72-iv83, 2017 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
