

Dysphagia due to anterior cervical osteophytosis: case report
- PMID: 34932659
- PMCID: PMC9927700
- DOI: 10.1590/2317-1782/20212020435
Dysphagia due to anterior cervical osteophytosis: case report
Abstract
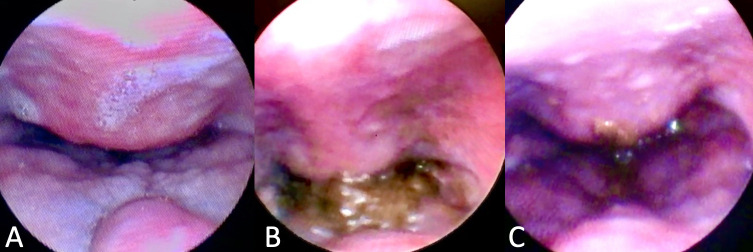
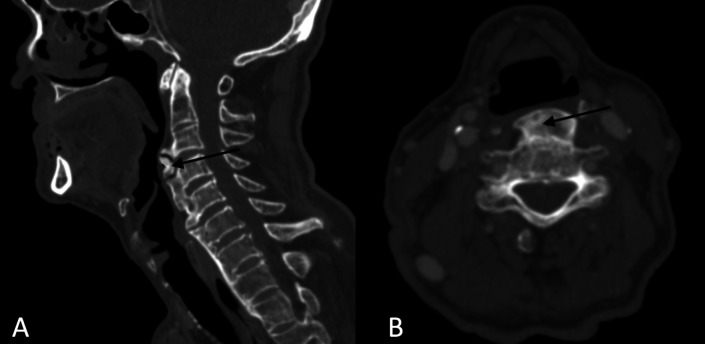
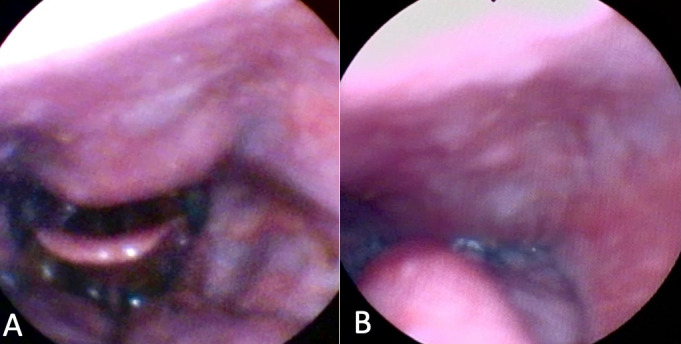
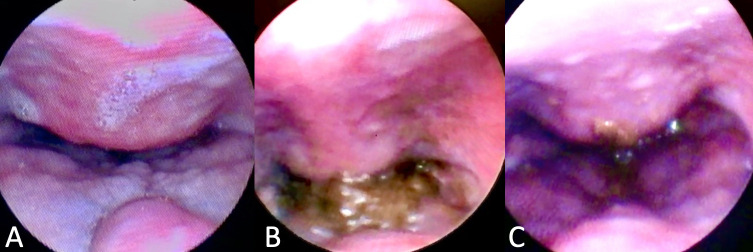
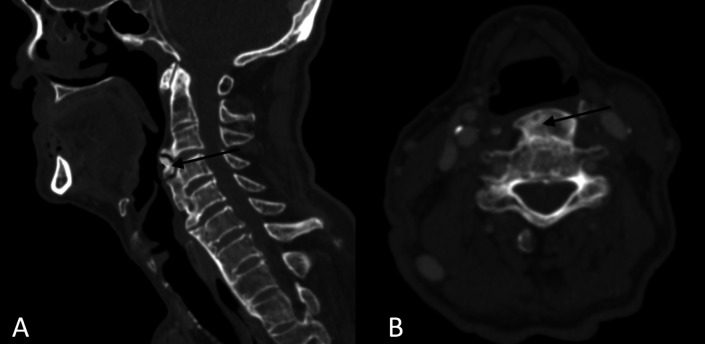
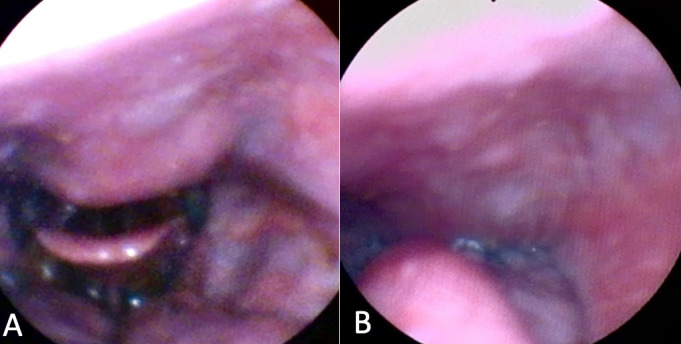
Anterior cervical osteophytosis is a noninflammatory condition characterized by calcification or ossification of the anterolateral paravertebral ligaments of the cervical spine. It affects 20 to 30% of the elderly, being responsible for 1.6% of the identifiable etiologies of dysphagia in the senile population. In advanced states, dysphagia due to cervical osteophytosis can lead to complications such as malnutrition, weight loss and aspiration pneumonia. This study aims to alert to this diagnosis, enabling early treatment of the condition. The case of a 66-year-old male patient with choking dysphagia for solids and nasal food reflux for 1 year is reported. Fiberoptic Endoscopic Evaluation of Swallowing showed bulging of the posterior pharyngeal wall and, with solid food supply, restriction to the retroflexion of the epiglottis, nasal reflux of the food and a large amount of food residue on the lesion. Cervical spine Computed Tomography identified the presence of anterior cervical osteophytes between the C3 and C6 vertebrae, the largest with anteroposterior length of 12 millimeters, narrowing the air column at the level of the oro- and hypopharynx. The patient was adequately treated with swallowing therapy by speech-language pathologist. The initial treatment strategy for symptomatic osteophytosis should be conservative, usually with a good response to swallowing therapy. Although they are rarely implicated in the etiology of dysphagia, considering its high prevalence, it is important that otolaryngologists and speech-language pathologists are attentive to this diagnosis, allowing early and effective treatment for the assisted patient, better prognosis and fewer complications of oropharyngeal dysphagia in the elderly.
Osteofitose cervical anterior é uma condição não inflamatória caracterizada por calcificação ou ossificação dos ligamentos paravertebrais anterolaterais da coluna cervical. Acomete 20 a 30% dos idosos, sendo responsável por 1,6% das etiologias identificáveis da disfagia na população senil. Em estados avançados, a disfagia por osteofitose cervical pode levar a complicações como desnutrição, perda de peso e pneumonia aspirativa. Este estudo visa alertar para a suspeição desse diagnóstico à equipe multidisciplinar que cuida do idoso disfágico, possibilitando tratamento oportuno e precoce da condição. É relatado o caso de um paciente masculino de 66 anos com disfagia tipo engasgo para sólidos e refluxo nasal de alimentos há 1 ano. Videoendoscopia da deglutição evidenciou abaulamento da parede posterior da faringe e, à oferta de alimento sólido, restrição à retroflexão da epiglote, refluxo nasal do alimento e grande quantidade de resíduo alimentar sobre a lesão. Tomografia computadorizada de coluna cervical identificou a presença de osteófitos cervicais anteriores entre as vértebras C3 e C6, o maior com comprimento anteroposterior de 12 milímetros, estreitando a coluna aérea ao nível da oro- e hipofaringe. O paciente foi adequadamente tratado com fonoterapia da deglutição. A estratégia inicial de tratamento para a osteofitose sintomática deve ser conservadora, geralmente com boa resposta à fonoterapia da deglutição. Apesar de raramente estarem implicados na etiologia da disfagia, considerando sua alta prevalência, é importante que otorrinolaringologistas e fonoaudiólogos estejam atentos a esse diagnóstico, permitindo tratamento precoce e efetivo para o paciente assistido, melhor prognóstico e menos complicações da disfagia orofaríngea no idoso.
RESUMO: Osteofitose cervical anterior é uma condição não inflamatória caracterizada por calcificação ou ossificação dos ligamentos paravertebrais anterolaterais da coluna cervical. Acomete 20 a 30% dos idosos, sendo responsável por 1,6% das etiologias identificáveis da disfagia na população senil. Em estados avançados, a disfagia por osteofitose cervical pode levar a complicações como desnutrição, perda de peso e pneumonia aspirativa. Este estudo visa alertar para a suspeição desse diagnóstico à equipe multidisciplinar que cuida do idoso disfágico, possibilitando tratamento oportuno e precoce da condição. É relatado o caso de um paciente masculino de 66 anos com disfagia tipo engasgo para sólidos e refluxo nasal de alimentos há 1 ano. Videoendoscopia da deglutição evidenciou abaulamento da parede posterior da faringe e, à oferta de alimento sólido, restrição à retroflexão da epiglote, refluxo nasal do alimento e grande quantidade de resíduo alimentar sobre a lesão. Tomografia computadorizada de coluna cervical identificou a presença de osteófitos cervicais anteriores entre as vértebras C3 e C6, o maior com comprimento anteroposterior de 12 milímetros, estreitando a coluna aérea ao nível da oro- e hipofaringe. O paciente foi adequadamente tratado com fonoterapia da deglutição. A estratégia inicial de tratamento para a osteofitose sintomática deve ser conservadora, geralmente com boa resposta à fonoterapia da deglutição. Apesar de raramente estarem implicados na etiologia da disfagia, considerando sua alta prevalência, é importante que otorrinolaringologistas e fonoaudiólogos estejam atentos a esse diagnóstico, permitindo tratamento precoce e efetivo para o paciente assistido, melhor prognóstico e menos complicações da disfagia orofaríngea no idoso.
Conflict of interest statement
Conflict of interests: nothing to declare.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
