

Predictors of Severe Acute Respiratory Syndrome Coronavirus 2 Infection Following High-Risk Exposure
- PMID: 34932817
- PMCID: PMC8903328
- DOI: 10.1093/cid/ciab1040
Predictors of Severe Acute Respiratory Syndrome Coronavirus 2 Infection Following High-Risk Exposure
Abstract
Background: Non-pharmaceutical interventions (NPIs) are recommended for COVID-19 prevention. However, the effectiveness of NPIs in preventing SARS-CoV-2 transmission remains poorly quantified.
Methods: We conducted a test-negative design case-control study enrolling cases (testing positive for SARS-CoV-2) and controls (testing negative) with molecular SARS-CoV-2 diagnostic test results reported to California Department of Public Health between 24 February-12 November, 2021. We used conditional logistic regression to estimate adjusted odds ratios (aORs) of case status among participants who reported contact with an individual known or suspected to have been infected with SARS-CoV-2 ("high-risk exposure") ≤14 days before testing.
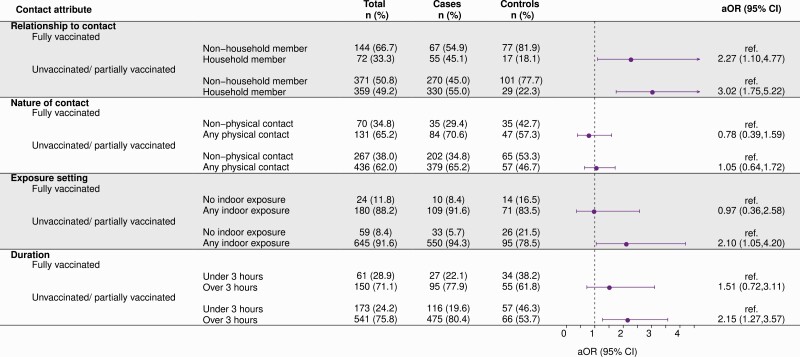
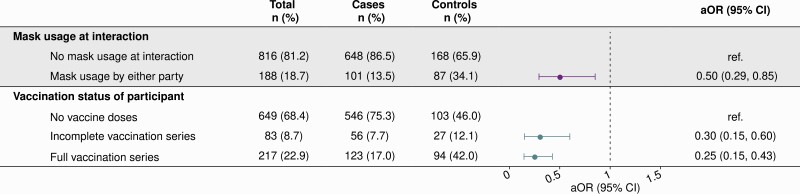
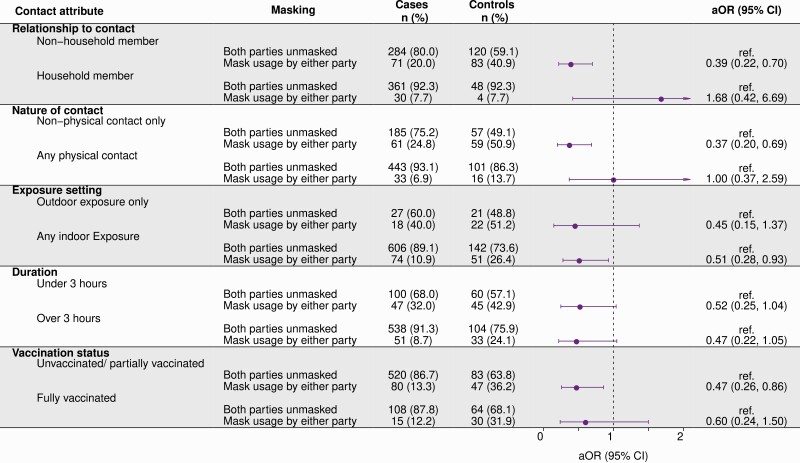
Results: 751 of 1448 cases (52%) and 255 of 1443 controls (18%) reported high-risk exposures ≤14 days before testing. Adjusted odds of case status were 3.02-fold (95% confidence interval: 1.75-5.22) higher when high-risk exposures occurred with household members (vs. other contacts), 2.10-fold (1.05-4.21) higher when exposures occurred indoors (vs. outdoors only), and 2.15-fold (1.27-3.67) higher when exposures lasted ≥3 hours (vs. shorter durations) among unvaccinated and partially-vaccinated individuals; excess risk associated with such exposures was mitigated among fully-vaccinated individuals. Cases were less likely than controls to report mask usage during high-risk exposures (aOR = 0.50 [0.29-0.85]). The adjusted odds of case status was lower for fully-vaccinated (aOR = 0.25 [0.15-0.43]) participants compared to unvaccinated participants. Benefits of mask usage were greatest among unvaccinated and partially-vaccinated participants, and in interactions involving non-household contacts or interactions occurring without physical contact.
Conclusions: NPIs reduced the likelihood of SARS-CoV-2 infection following high-risk exposure. Vaccine effectiveness was substantial for partially and fully vaccinated persons.
Keywords: SARS-CoV-2; face masks; non-pharmaceutical interventions; vaccination.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Haas EJ, Angulo FJ, McLaughlin JM, et al. . Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet 2021; 397:1819–29. - PMC - PubMed
-
- Jones NR, Qureshi ZU, Temple RJ, Larwood JPJ, Greenhalgh T, Bourouiba L.. Two metres or one: what is the evidence for physical distancing in covid-19?. BMJ 2020; 370:m3223. - PubMed
