

Association Between Age and Outcomes of Catheter Ablation Versus Medical Therapy for Atrial Fibrillation: Results From the CABANA Trial
- PMID: 34933570
- PMCID: PMC9003625
- DOI: 10.1161/CIRCULATIONAHA.121.055297
Association Between Age and Outcomes of Catheter Ablation Versus Medical Therapy for Atrial Fibrillation: Results From the CABANA Trial
Abstract
Background: Observational data suggest that catheter ablation may be safe and effective to treat younger and older patients with atrial fibrillation. No large, randomized trial has examined this issue. This report describes outcomes according to age at entry in the CABANA trial (Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation).
Methods: Patients with atrial fibrillation ≥65 years of age, or <65 with ≥1 risk factor for stroke, were randomly assigned to catheter ablation versus drug therapy. The primary outcome was a composite of death, disabling stroke, serious bleeding, or cardiac arrest. Secondary outcomes included all-cause mortality, the composite of mortality or cardiovascular hospitalization, and recurrence of atrial fibrillation. Treatment effect estimates were adjusted for baseline covariables using proportional hazards regression models.
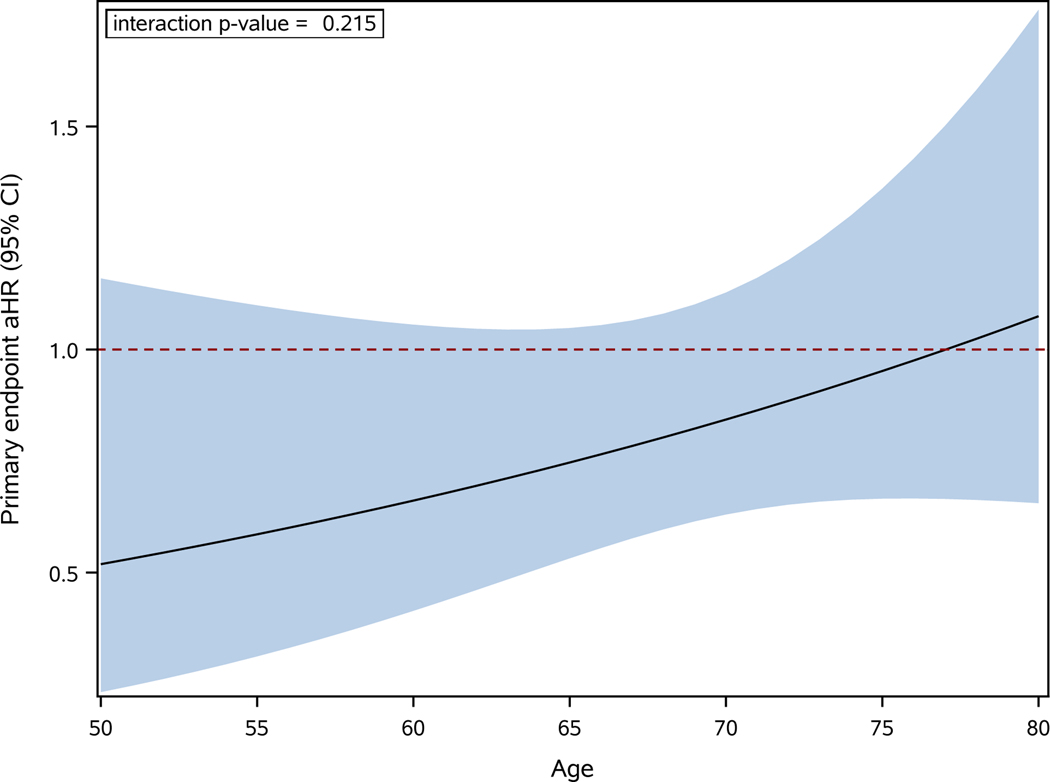
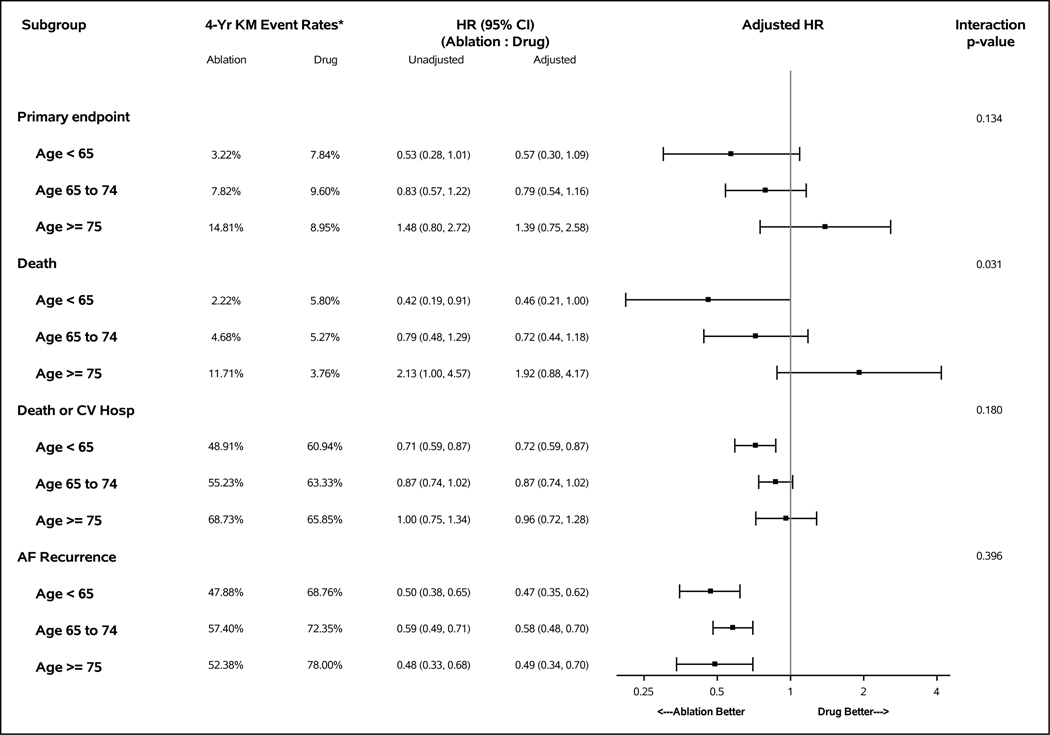
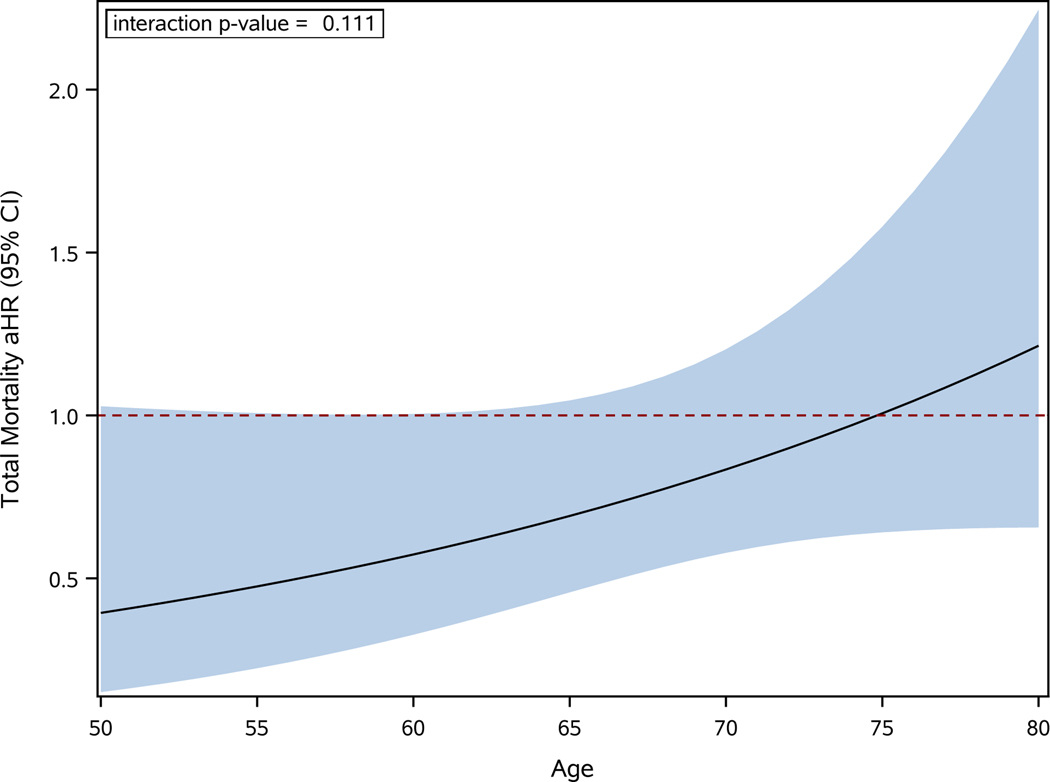
Results: Of 2204 patients randomly assigned in CABANA, 766 (34.8%) were <65 years of age, 1130 (51.3%) were 65 to 74 years of age, and 308 (14.0%) were ≥75 years of age. Catheter ablation was associated with a 43% reduction in the primary outcome for patients <65 years of age (adjusted hazard ratio [aHR], 0.57 [95% CI, 0.30-1.09]), a 21% reduction for 65 to 74 years of age (aHR, 0.79 [95% CI, 0.54-1.16]), and an indeterminate effect for age ≥75 years of age (aHR, 1.39 [95% CI, 0.75-2.58]). Four-year event rates for ablation versus drug therapy across age groups, respectively, were 3.2% versus 7.8%, 7.8% versus 9.6%, and 14.8% versus 9.0%. For every 10-year increase in age, the primary outcome aHR increased (ie, less favorable to ablation) an average of 27% (interaction P value=0.215). A similar pattern was seen with all-cause mortality: for every 10-year increase in age, the aHR increased an average of 46% (interaction P value=0.111). Atrial fibrillation recurrence rates were lower with ablation than with drug therapy across age subgroups (aHR 0.47, 0.58, and 0.49, respectively). Treatment-related complications were infrequent for both arms (<3%) regardless of age.
Conclusions: We found age-based variations in clinical outcomes for catheter ablation compared with drug therapy, with the largest relative and absolute benefits of catheter ablation in younger patients. No prognostic benefits for ablation were seen in the oldest patients. No differences were found by age in treatment-related complications or in the relative effectiveness of catheter ablation in preventing recurrent atrial arrhythmias.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT00911508.
Keywords: age groups; anti-arrhythmia agents; atrial fibrillation; catheter ablation; pulmonary veins.
Figures
Comment in
-
Atrial Fibrillation Ablation: Aiming to Improve Quantity and Quality of Life.Circulation. 2022 Mar 15;145(11):805-807. doi: 10.1161/CIRCULATIONAHA.121.058636. Epub 2022 Mar 14. Circulation. 2022. PMID: 35286168 No abstract available.
-
In AF, CV benefits of catheter ablation vs. medical therapy may vary by age.Ann Intern Med. 2022 Jul;175(7):JC77. doi: 10.7326/J22-0042. Epub 2022 Jul 5. Ann Intern Med. 2022. PMID: 35785544
References
-
- Jais P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, Hocini M, Extramiana F, Sacher F, Bordachar P, et al. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. Circulation. 2008;118:2498–505. - PubMed
-
- Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A, Macle L, Daoud EG, Calkins H, Hall B, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303:333–40. - PubMed
-
- Bunch TJ, Weiss JP, Crandall BG, May HT, Bair TL, Osborn JS, Anderson JL, Lappe DL, Muhlestein JB, Nelson J, et al. Long-term clinical efficacy and risk of catheter ablation for atrial fibrillation in octogenarians. Pacing Clin Electrophysiol. 2010;33:146–52. - PubMed
-
- Santangeli P, Di Biase L, Mohanty P, Burkhardt JD, Horton R, Bai R, Mohanty S, Pump A, Gibson D, Couts L, et al. Catheter ablation of atrial fibrillation in octogenarians: safety and outcomes. J Cardiovasc Electrophysiol. 2012;23:687–93. - PubMed
-
- Zado E, Callans DJ, Riley M, Hutchinson M, Garcia F, Bala R, Lin D, Cooper J, Verdino R, et al. Long-term clinical efficacy and risk of catheter ablation for atrial fibrillation in the elderly. J Cardiovasc Electrophysiol. 2008;19:621–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
