

Evaluation of pathological complete response as surrogate endpoint in neoadjuvant randomised clinical trials of early stage breast cancer: systematic review and meta-analysis
- PMID: 34933868
- PMCID: PMC8689398
- DOI: 10.1136/bmj-2021-066381
Evaluation of pathological complete response as surrogate endpoint in neoadjuvant randomised clinical trials of early stage breast cancer: systematic review and meta-analysis
Abstract
Objective: To evaluate pathological complete response as a surrogate endpoint for disease-free survival and overall survival in regulatory neoadjuvant trials of early stage breast cancer.
Design: Systematic review and meta-analysis.
Data sources: Medline, Embase, and Scopus to 1 December 2020.
Eligibility criteria for study selection: Randomised clinical trials that tested neoadjuvant chemotherapy given alone or combined with other treatments, including anti-human epidermal growth factor 2 (anti-HER2) drugs, targeted treatments, antivascular agents, bisphosphonates, and immune checkpoint inhibitors.
Data extraction and synthesis: Trial level associations between the surrogate endpoint pathological complete response and disease-free survival and overall survival.
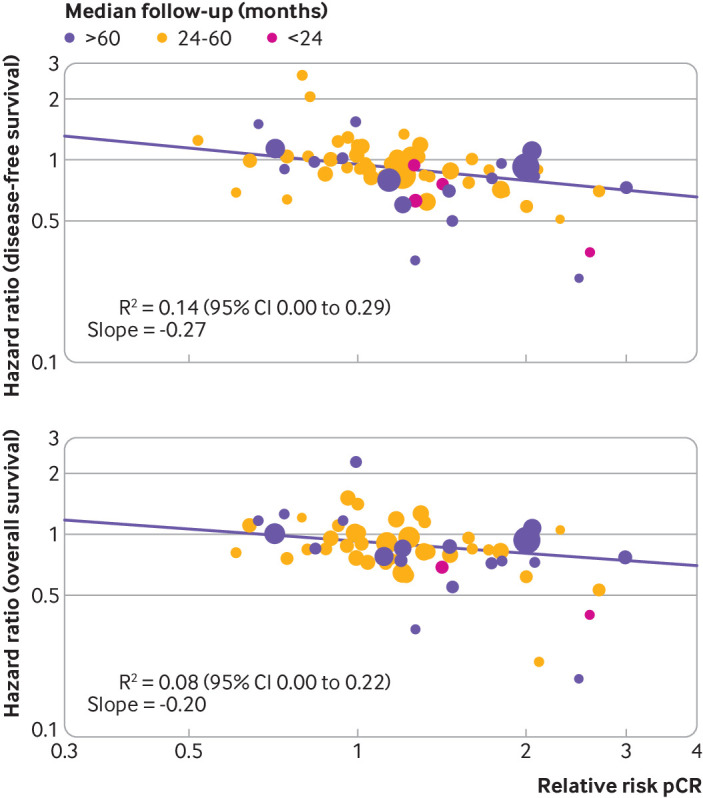
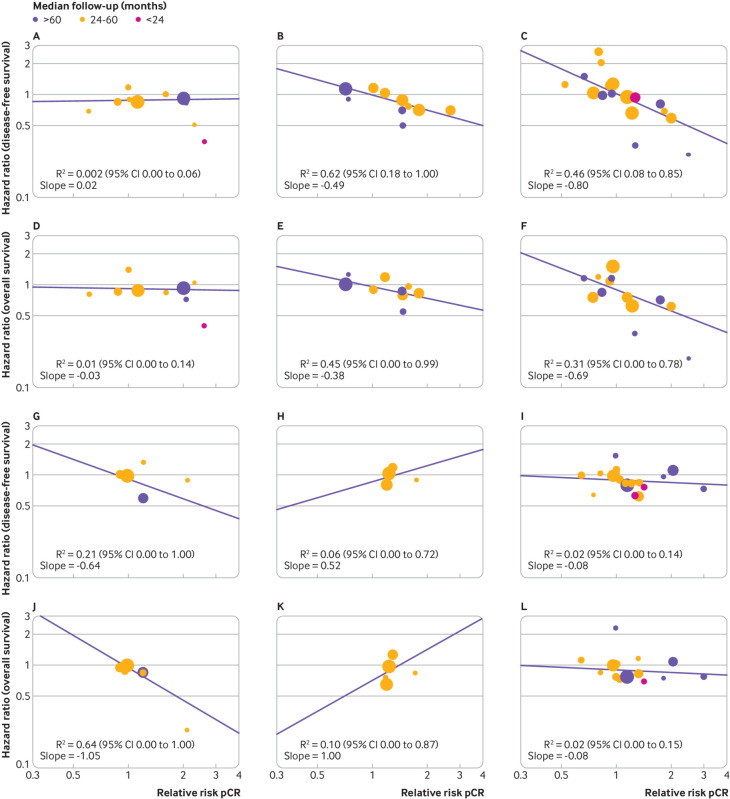
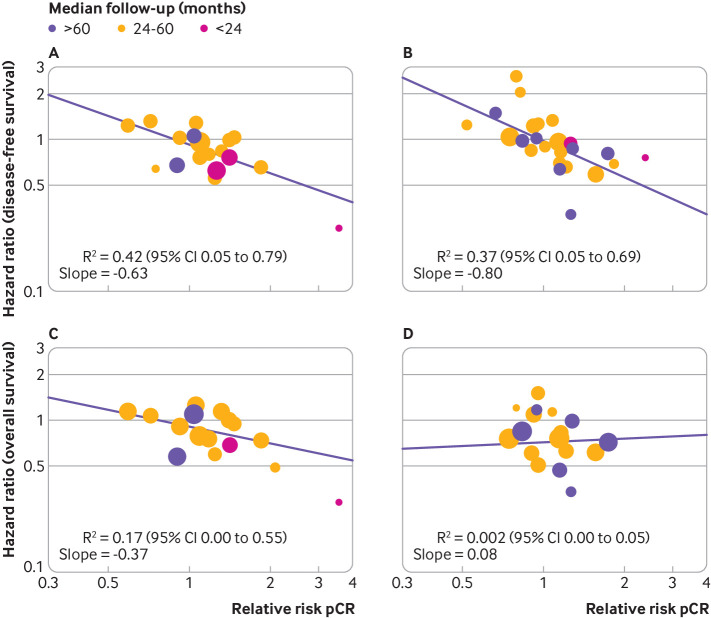
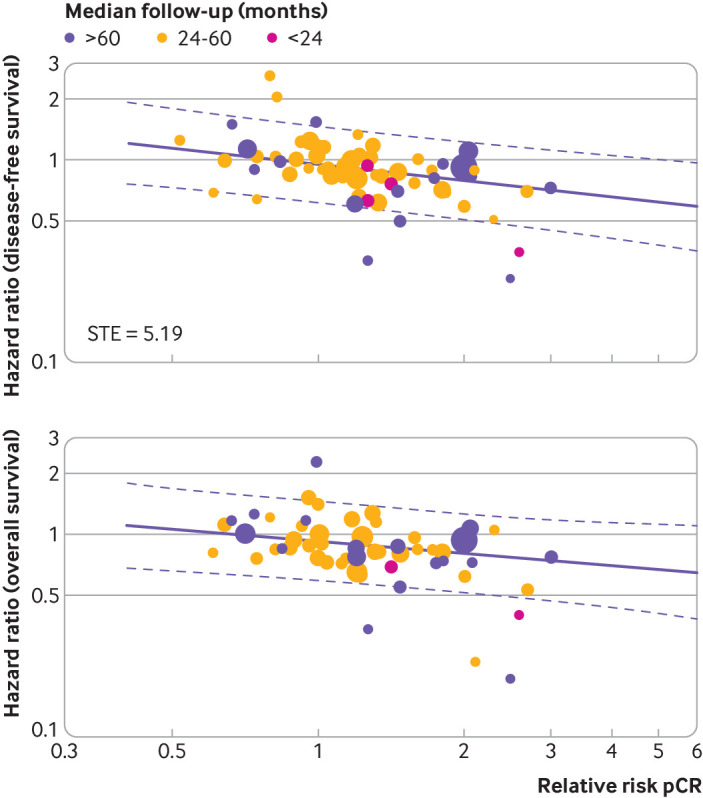
Methods: A weighted regression analysis was performed on log transformed treatment effect estimates (hazard ratio for disease-free survival and overall survival and relative risk for pathological complete response), and the coefficient of determination (R2) was used to quantify the association. The secondary objective was to explore heterogeneity of results in preplanned subgroups analysis, stratifying trials according treatment type in the experimental arm, definition used for pathological complete response (breast and lymph nodes v breast only), and biological features of the disease (HER2 positive or triple negative breast cancer). The surrogate threshold effect was also evaluated, indicating the minimum value of the relative risk for pathological complete response necessary to confidently predict a non-null effect on hazard ratio for disease-free survival or overall survival.
Results: 54 randomised clinical trials comprising a total of 32 611 patients were included in the analysis. A weak association was observed between the log(relative risk) for pathological complete response and log(hazard ratio) for both disease-free survival (R2=0.14, 95% confidence interval 0.00 to 0.29) and overall survival (R2 =0.08, 0.00 to 0.22). Similar results were found across all subgroups evaluated, independently of the definition used for pathological complete response, treatment type in the experimental arm, and biological features of the disease. The surrogate threshold effect was 5.19 for disease-free survival but was not estimable for overall survival. Consistent results were confirmed in three sensitivity analyses: excluding small trials (<200 patients enrolled), excluding trials with short median follow-up (<24 months), and replacing the relative risk for pathological complete response with the absolute difference of pathological complete response rates between treatment arms.
Conclusion: A lack of surrogacy of pathological complete response was identified at trial level for both disease-free survival and overall survival. The findings suggest that pathological complete response should not be used as primary endpoint in regulatory neoadjuvant trials of early stage breast cancer.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- US Department of Health and Human Services. US Food and Drug Ad- ministration, Center for Drug Evaluation and Research (CDER): Guidance for Industry: Pathological Complete Response in Neoadjuvant Treatment of High-Risk Early-Stage Breast Cancer—Use as an Endpoint to Support Accelerated Approval. www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guid...
-
- European Medicines Agency. EMA/CHMP/ 151853/2014: Draft guideline on the role of the pathological complete response as an endpoint in neoadjuvant breast cancer studies. www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2014/...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous