

The 2018 Global Point Prevalence Survey of antimicrobial consumption and resistance in 47 Canadian hospitals: a cross-sectional survey
- PMID: 34933882
- PMCID: PMC8695542
- DOI: 10.9778/cmajo.20200274
The 2018 Global Point Prevalence Survey of antimicrobial consumption and resistance in 47 Canadian hospitals: a cross-sectional survey
Abstract
Background: Patient-level surveillance of antimicrobial use (AMU) in Canadian hospitals empowers the reduction of inappropriate AMU and was piloted in 2017 among 14 hospitals in Canada. We aimed to describe AMU on the basis of patient-level data in Canadian hospitals in 2018 in terms of antimicrobial prescribing prevalence and proportions, antimicrobial indications, and agent selection in medical, surgical and intensive care wards.
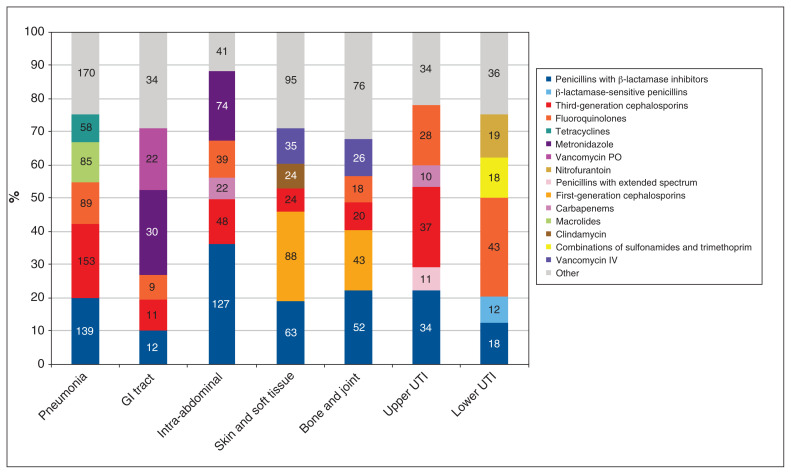
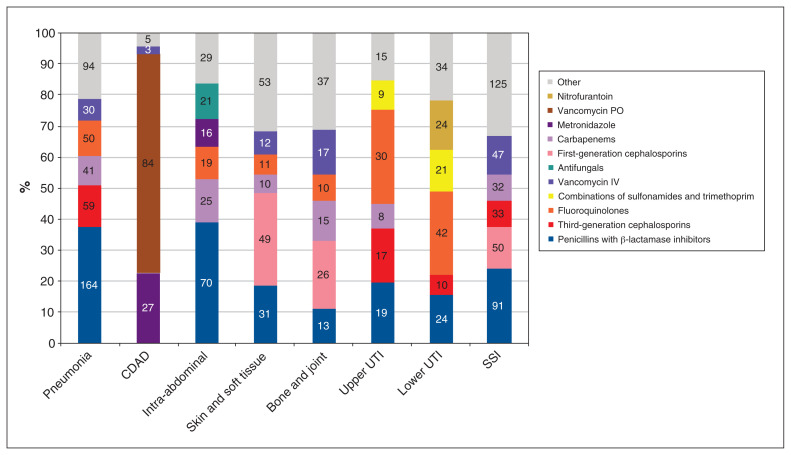
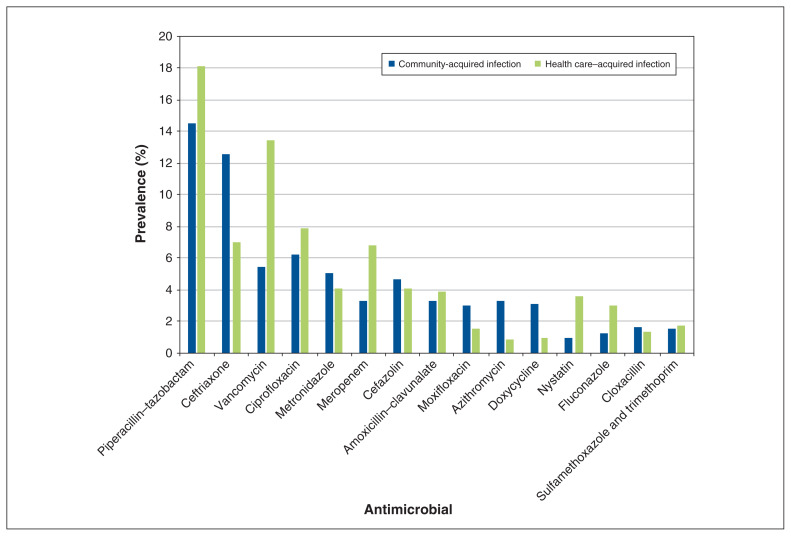
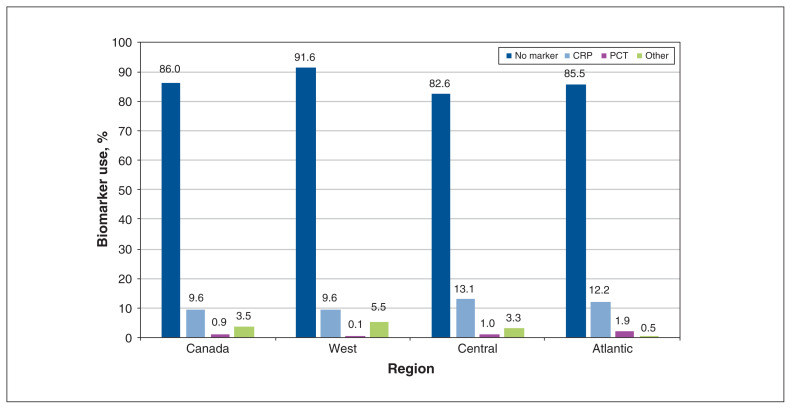
Methods: Canadian adult, pediatric and neonatal hospitals were invited to participate in the standardized web-based cross-sectional Global Point Prevalence Survey of Antimicrobial Consumption and Resistance (Global-PPS) conducted in 2018. An identified site administrator assigned all wards admitting inpatients to specific surveyors. A physician, pharmacist or nurse with infectious disease training performed the survey. The primary outcomes were point prevalence rates for AMU over the study period regarding prescriptions, indications and agent selection in medical, surgical and intensive care wards. The secondary outcomes were AMU for resistant organisms and practice appropriateness evaluated on the basis of quality indicators. Antimicrobial consumption is presented in terms of prevalence and proportions.
Results: Forty-seven of 118 (39.8%) hospitals participated in the survey; 9 hospitals were primary care centres, 15 were secondary care centres and 23 were tertiary or specialized care centres. Of 13 272 patients included, 33.5% (n = 4447) received a total of 6525 antimicrobials. Overall, 74.1% (4832/6525) of antimicrobials were for therapeutic use, 12.6% (n = 825) were for medical prophylaxis, 8.9% (n = 578) were for surgical prophylaxis, 2.2% (n = 143) were for other use and 2.3% (n = 147) were for unidentified reasons. A diagnosis or indication was documented in the patient's file at the initiation for 87.3% (n = 5699) of antimicrobials; 62.9% (n = 4106) of antimicrobials had a stop or review date; and 72.0% (n = 4697) of prescriptions were guided by local guidelines.
Interpretation: Overall, three-quarters of AMU was for therapeutic use across participating hospitals. Canadian hospitals should be further incentivized to create and adapt local guidelines on the basis of recent antimicrobial resistance data.
© 2021 CMA Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Daniel Thirion has shares in Lumed. No other competing interests were declared.
Figures
References
-
- Abat C, Rolain JM, Dubourg G, et al. Evaluating the clinical burden and mortality attributable to antibiotic resistance: the disparity of empirical data and simple model estimations. Clin Infect Dis. 2017;65(Suppl 1):S58–63. - PubMed
-
- Global action plan on antimicrobial resistance. Geneva: World Health Organization; 2015. [accessed 2021 Apr. 16]. Available: www.who.int/antimicrobial-resistance/global-action-plan/en/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical