

Bifurcation functional significance score as predictor of mortality: a validating study
- PMID: 34934122
- PMCID: PMC8692595
- DOI: 10.1038/s41598-021-03815-6
Bifurcation functional significance score as predictor of mortality: a validating study
Abstract
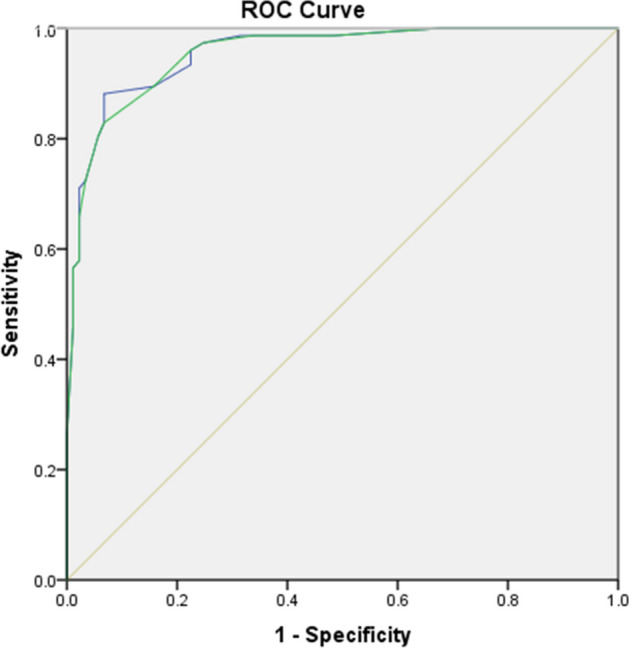
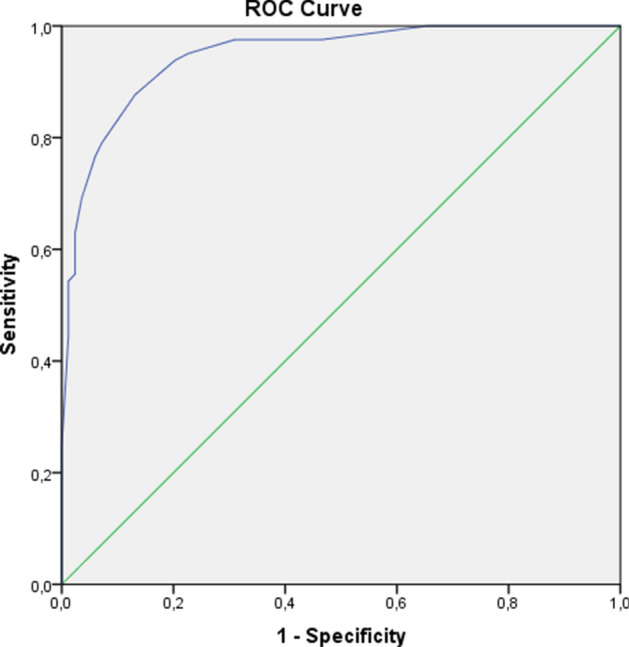
Considerable progress has been made in the treatment of coronary bifurcation stenosis. Anatomical characteristics of the vessel and lesion, however, fail to give information about the functional significance of the bifurcation stenosis. To the best of our knowledge, there is no study that systematically establishes the baseline functional significance of coronary stenosis and its effect on procedural and clinical outcomes. Patients with significant angiographic bifurcation lesions defined as diameter stenosis > 50% in main vessel and/or side branch were included. FFR was performed in main vessel (MV) and side branch (SB) before and after percutaneous coronary intervention (PCI). 169 patients from Fiesta study (derivation cohort) and 555 patients from prospective bifurcation registry (clinical effect cohort) were analyzed to validate angiographic prediction score (BFSS) used to determine the potentially functional significance of coronary bifurcation stenosis. Bifurcation functional significance score (including the following parameters-SYNTAX ≥ 11, SB/MB BARI score, MV %DS ≥ 55%, main branch (MB) %DS ≥ 65%, lesion length ≥ 25 mm) with a maximum value of 11 was developed. A cut-off value of 6.0 was shown to give the best discriminatory ability-with accuracy 87% (sensitivity 77%, specificity 96%, p < 0.001). There was also a significant difference in all-cause mortality between patients with BFSS ≥ 6.0 vs. BFSS < 6.0-25.5% vs. 18.4%, log-rank p = 0.001 as well as cardiac mortality: BFSS ≥ 6.0 vs. BFSS < 6.0-17.7% vs. 14.5%, log-rank (p = 0.016). The cardiac mortality was significantly lower in patients with smaller absolute SB territory, p = 0.023. An angiographic score (BFSS) with good discriminatory ability to determine the functional significance of coronary bifurcation stenosis was developed. The value for BFSS ≥ 6.0 can be used as a discriminator to define groups with higher risk for all-cause and cardiac mortality. Also, we found that the smaller side branches pose greater mortality risk.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
