

Differential Impact of the COVID-19 Pandemic on Health Care Utilization Disruption for Community-Dwelling Individuals With and Without Acquired Brain Injury
- PMID: 34934940
- PMCID: PMC8677629
- DOI: 10.1016/j.arrct.2021.100176
Differential Impact of the COVID-19 Pandemic on Health Care Utilization Disruption for Community-Dwelling Individuals With and Without Acquired Brain Injury
Erratum in
-
Correction.Arch Rehabil Res Clin Transl. 2022 Jul 27;4(3):100222. doi: 10.1016/j.arrct.2022.100222. eCollection 2022 Sep. Arch Rehabil Res Clin Transl. 2022. PMID: 36123977 Free PMC article.
Abstract
Objective: To delineate health care disruption for individuals with acquired brain injury (ABI) during the peak of the pandemic and to understand the impact of health care disruption on health-related quality of life (HRQoL).
Design: Cross-sectional survey.
Setting: General community.
Participants: Volunteer sample of adults with traumatic brain injury (TBI; n=33), adults with stroke (n=66), and adults without TBI or stroke (n=108) with access to the internet and personal technology (N=207).
Interventions: Not applicable.
Main outcome measures: Not applicable.
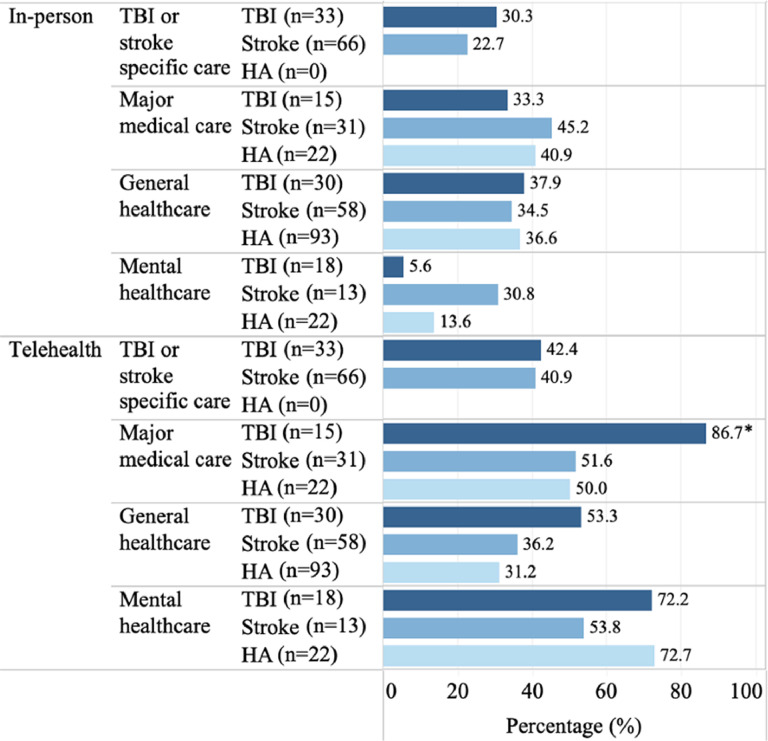
Results: Participants with TBI and stroke reported high rates of disruption in care specific to their diagnosis (53%-54.5%), while participants across all groups reported disruption for major medical care (range, 68.2%-80%), general health care (range, 60.3%-72.4%), and mental health care (range, 31.8%-83.3%). During the pandemic, participants with TBI and stroke used telehealth for care specific to their diagnosis (40.9%-42.4%), whereas all participants used telehealth for major medical care (range, 50%-86.7%), general health care (range, 31.2%-53.3%), and mental health care (range, 53.8%-72.7%). Disruption in TBI or stroke care and type of ABI explained 27.1% of the variance in HRQoL scores (F2,95=16.82, P<.001, R 2=0.262), and disruption in mental health care explained 14.8% of the variance (F1,51=8.86, P=.004, R 2=0.148).
Conclusions: Individuals with and without ABI experienced pronounced disruption in health care utilization overall. However, individuals who experienced a disruption in care specific to TBI or mental health care were most vulnerable to decreased HRQoL. Telehealth was a viable alternative to in-person visits for individuals with and without ABI, but limitations included difficulty with technology, difficulty with comprehensive examination, and decreased rapport with providers.
Keywords: ABI, acquired brain injury; ANOVA, analysis of variance; Brain injuries, traumatic; COVID-19; HRQoL, health-related quality of life; Healthcare disparities; Patient acceptance of health care; Quality of life; Rehabilitation; Stroke; TBI, traumatic brain injury; Telemedicine.
© 2021 The Authors.
Figures


References
LinkOut - more resources
Full Text Sources
Miscellaneous
