

Emapalumab in primary haemophagocytic lymphohistiocytosis and the pathogenic role of interferon gamma: A pharmacometric model-based approach
- PMID: 34935183
- PMCID: PMC9305196
- DOI: 10.1111/bcp.15133
Emapalumab in primary haemophagocytic lymphohistiocytosis and the pathogenic role of interferon gamma: A pharmacometric model-based approach
Abstract
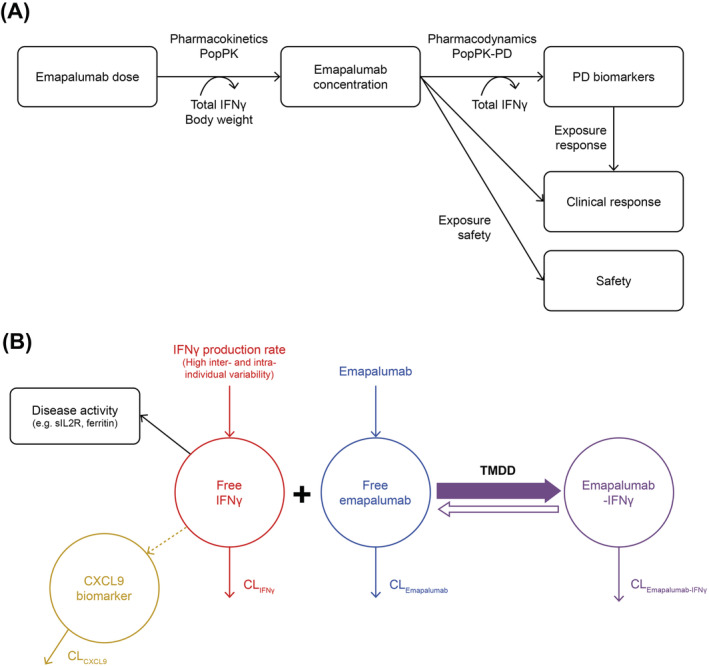
Aim: Primary haemophagocytic lymphohistiocytosis (HLH) is a rare, life-threatening, hyperinflammatory syndrome generally occurring in early childhood. The monoclonal antibody emapalumab binds and neutralises interferon γ (IFNγ). This study aimed to determine an emapalumab dosing regimen when traditional dose-finding approaches are not applicable, using pharmacokinetic-pharmacodynamic analyses to further clarify HLH pathogenesis and confirm IFNγ neutralisation as the relevant therapeutic target in pHLH.
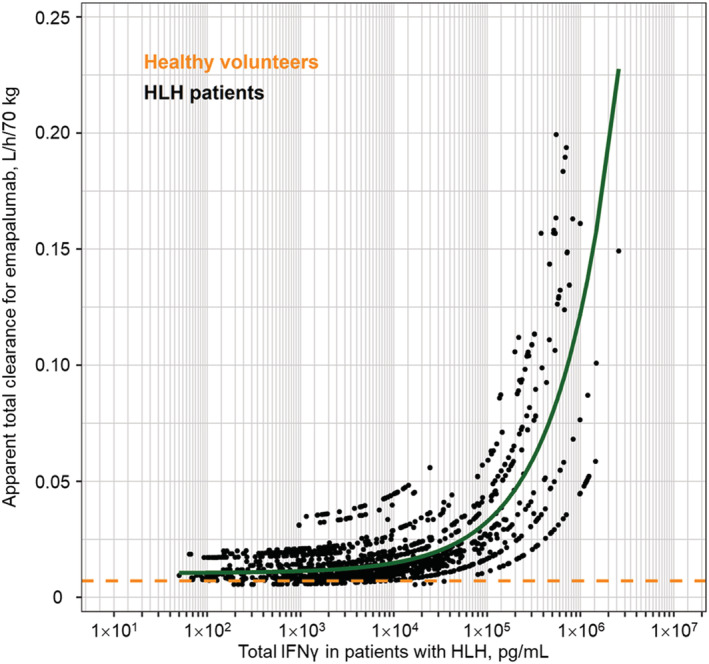
Methods: Initial emapalumab dosing (1 mg/kg) for pHLH patients participating in a pivotal multicentre, open-label, single-arm, phase 2/3 study was based on anticipated IFNγ levels and allometrically scaled pharmacokinetic parameters estimated in healthy volunteers. Emapalumab dosing was adjusted based on estimated IFNγ-mediated clearance and HLH clinical and laboratory criteria. Frequent dosing and emapalumab dose adaptation were used to account for highly variable IFNγ levels and potential target-mediated drug disposition.
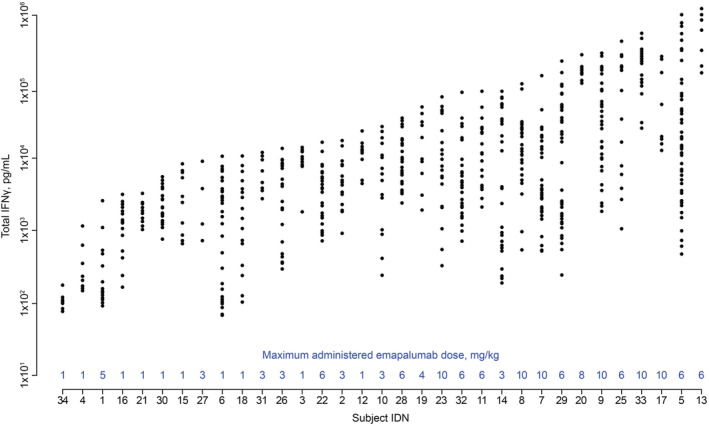
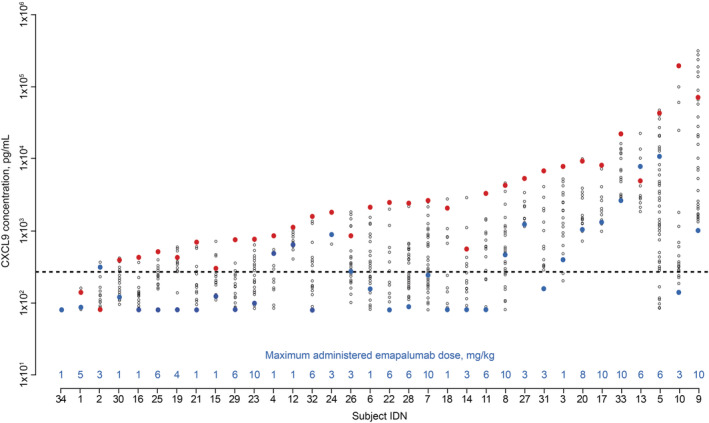
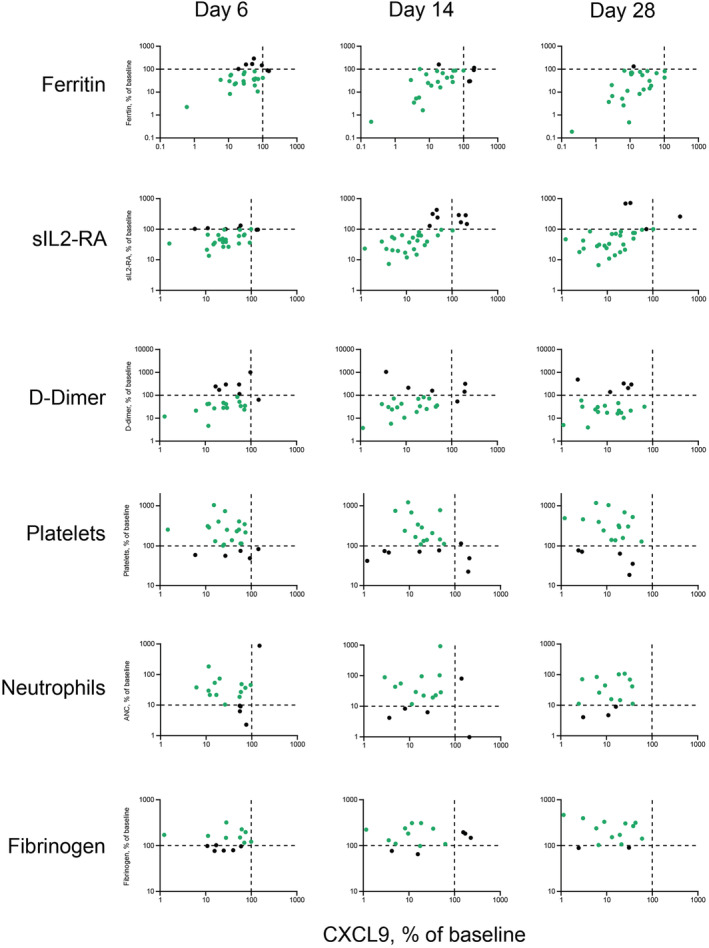
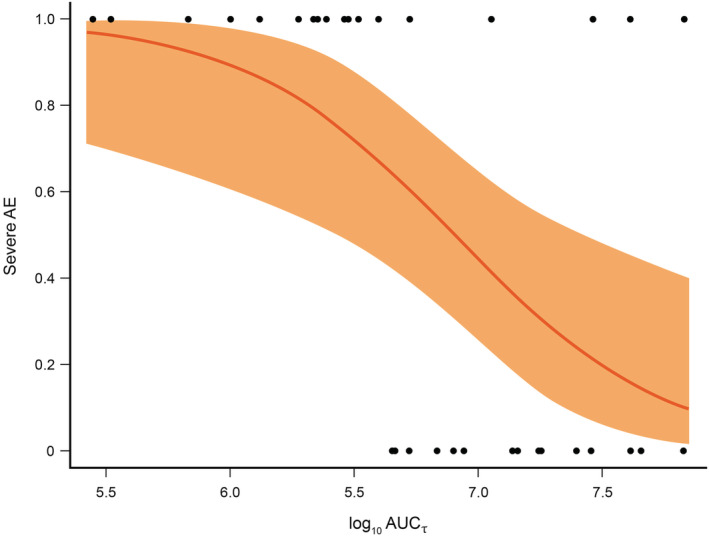
Results: High inter- and intra-individual variability in IFNγ production (assessed by total IFNγ levels, range: 102 -106 pg/mL) was observed in pHLH patients. Administering emapalumab reduced IFNγ activity, resulting in significant improvements in clinical and laboratory parameters and a reduced risk of adverse events, mainly related to pHLH. Modelled outcomes supported dose titration starting from 1 mg/kg, with possible increases to 3, 6 or 10 mg/kg based on re-evaluation of parameters of disease activity every 3 days.
Conclusions: The variable and unanticipated extremely high IFNγ concentrations in patients with pHLH are reflected in parameters of disease activity. Improved outcomes can be achieved by neutralising IFNγ using frequent emapalumab dosing and dose adaptation guided by clinical and laboratory observations.
Keywords: immunology - inflammation; immunology - monoclonal antibodies; paediatrics - children; pharmacodynamics - modelling and simulation; pharmacodynamics - pharmacokinetics-pharmacodynamics.
© 2021 Swedish Orphan Biovitrum AB (publ). British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
P.J., C.L., E.S., M.B.J., M.B. and C.dM. are paid consultants of Sobi. M.B.J. has participated in scientific advisory board meetings for Sobi. F.L. has acted as an unpaid consultant to Sobi, reviewing efficacy and safety data from clinical studies. M.B. and C.dM. are former employees of Sobi.
Figures
References
-
- Henter JI, Samuelsson‐Horne A, Aricò M, et al. Treatment of hemophagocytic lymphohistiocytosis with HLH‐94 immunochemotherapy and bone marrow transplantation. Blood. 2002;100(7):2367‐2373. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
