

Maternal Phthalates Exposure and Blood Pressure during and after Pregnancy in the PROGRESS Study
- PMID: 34935432
- PMCID: PMC8693773
- DOI: 10.1289/EHP8562
Maternal Phthalates Exposure and Blood Pressure during and after Pregnancy in the PROGRESS Study
Abstract
Background: Phthalate exposure is ubiquitous and may affect biological pathways related to regulators of blood pressure. Given the profound changes in vasculature during pregnancy, pregnant women may be particularly susceptible to the potential effects of phthalates on blood pressure.
Objectives: We examined associations of phthalate exposure during pregnancy with maternal blood pressure trajectories from mid-pregnancy through 72 months postpartum.
Methods: Women with singleton pregnancies delivering a live birth in Mexico City were enrolled during the second trimester (). Spot urine samples from the second and third trimesters were analyzed for 15 phthalate metabolites. Blood pressure and covariate data were collected over nine visits through 72 months postpartum. We used linear, logistic, and linear mixed models; latent class growth models (LCGMs); and Bayesian kernel machine regression to estimate the relationship of urinary phthalate biomarkers with maternal blood pressure.
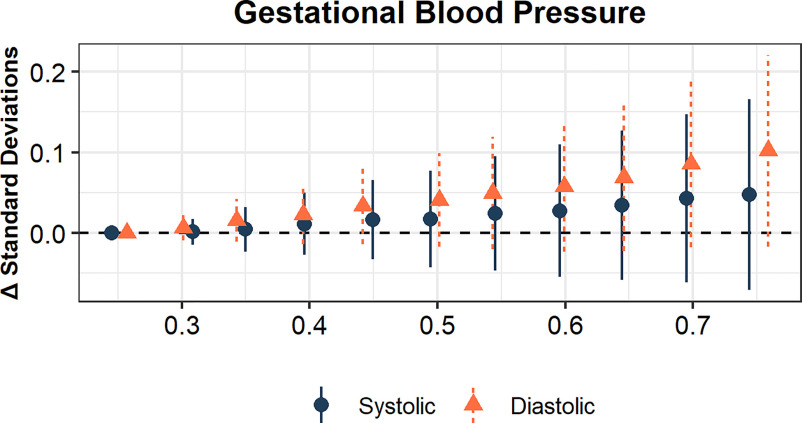
Results: As a joint mixture, phthalate biomarker concentrations during pregnancy were associated with higher blood pressure rise during mid-to-late gestation. With respect to individual biomarkers, second trimester concentrations of monobenzyl phthalate (MBzP) and di(2-ethylhexyl) phthalate biomarkers () were associated with higher third trimester blood pressure. Two trajectory classes were identified by LCGM, characterized by increasing blood pressure through 72 months postpartum ("increase-increase") or decreased blood pressure through 18 months postpartum with a gradual increase thereafter ("decrease-increase"). Increasing exposure to phthalate mixtures during pregnancy was associated with higher odds of being in the increase-increase class. Similar associations were observed for mono-2-ethyl-5-carboxypentyl terephthalate (MECPTP) and dibutyl phthalate () biomarkers. When specific time periods were examined, we observed specific temporal relationships were observed for , MECPTP, MBzP, and .
Discussion: In our cohort of pregnant women from Mexico City, exposure to phthalates and phthalate biomarkers was associated with higher blood pressure during late pregnancy, as well as with long-term changes in blood pressure trajectories. https://doi.org/10.1289/EHP8562.
Figures






Comment in
-
Invited Perspective: Phthalates and Blood Pressure: the Unknowns of Dietary Factors.Environ Health Perspect. 2021 Dec;129(12):121303. doi: 10.1289/EHP10172. Epub 2021 Dec 22. Environ Health Perspect. 2021. PMID: 34935433 Free PMC article. No abstract available.
References
-
- Amin MM, Ebrahimpour K, Parastar S, Shoshtari-Yeganeh B, Hashemi M, Mansourian M, et al. . 2018. Association of urinary concentrations of phthalate metabolites with cardiometabolic risk factors and obesity in children and adolescents. Chemosphere 211:547–556, PMID: , 10.1016/j.chemosphere.2018.07.172. - DOI - PubMed
-
- Bakk Z, Tekle FB, Vermunt JK. 2013. Estimating the association between latent class membership and external variables using bias-adjusted three-step approaches. Sociol Methodol 43(1):272–311, 10.1177/0081175012470644. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
