

The Effect of Advanced Age on the Electrode-Neuron Interface in Cochlear Implant Users
- PMID: 34935648
- PMCID: PMC9209609
- DOI: 10.1097/AUD.0000000000001185
The Effect of Advanced Age on the Electrode-Neuron Interface in Cochlear Implant Users
Abstract
Objectives: This study aimed to determine the effect of advanced age on how effectively a cochlear implant (CI) electrode stimulates the targeted cochlear nerve fibers (i.e., the electrode-neuron interface [ENI]) in postlingually deafened adult CI users. The study tested the hypothesis that the quality of the ENI declined with advanced age. It also tested the hypothesis that the effect of advanced age on the quality of the ENI would be greater in basal regions of the cochlea compared to apical regions.
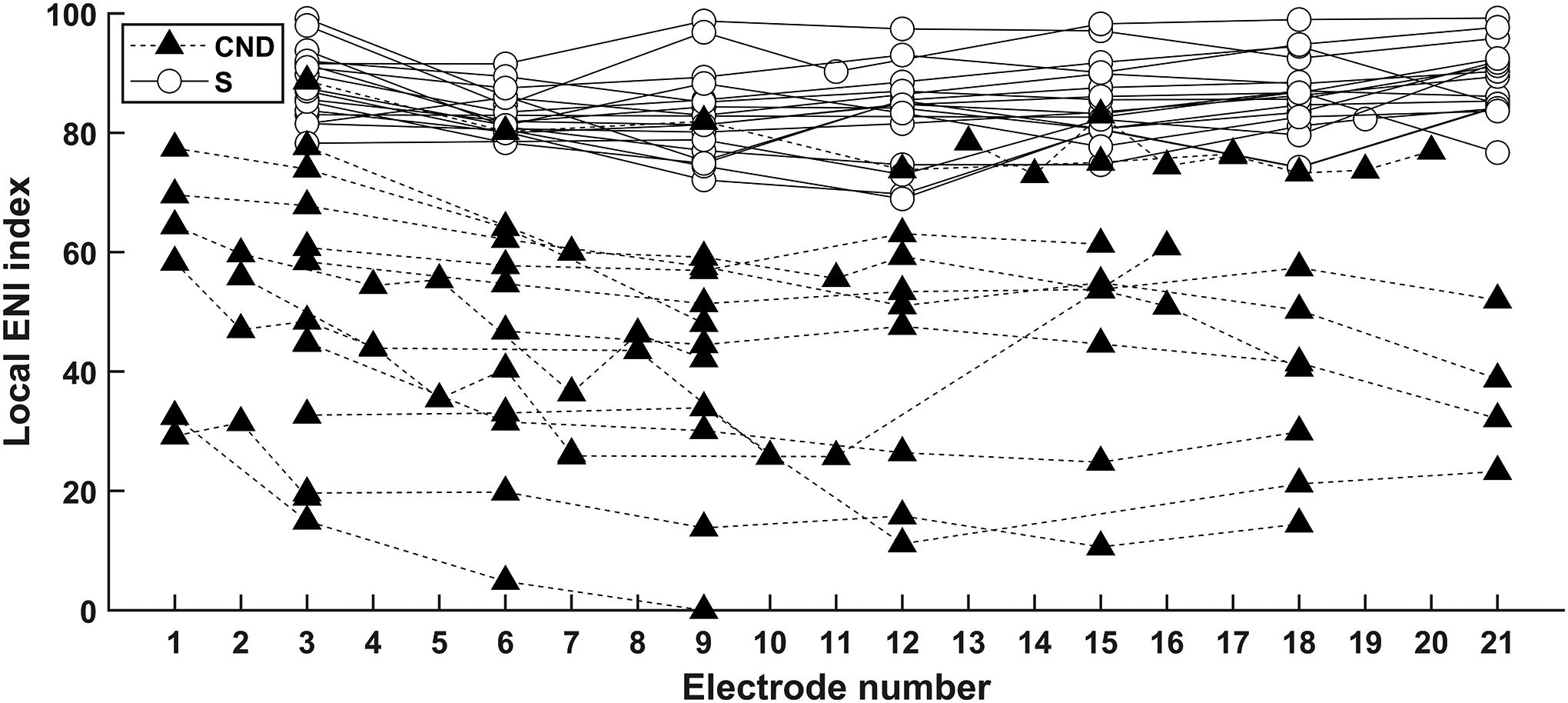
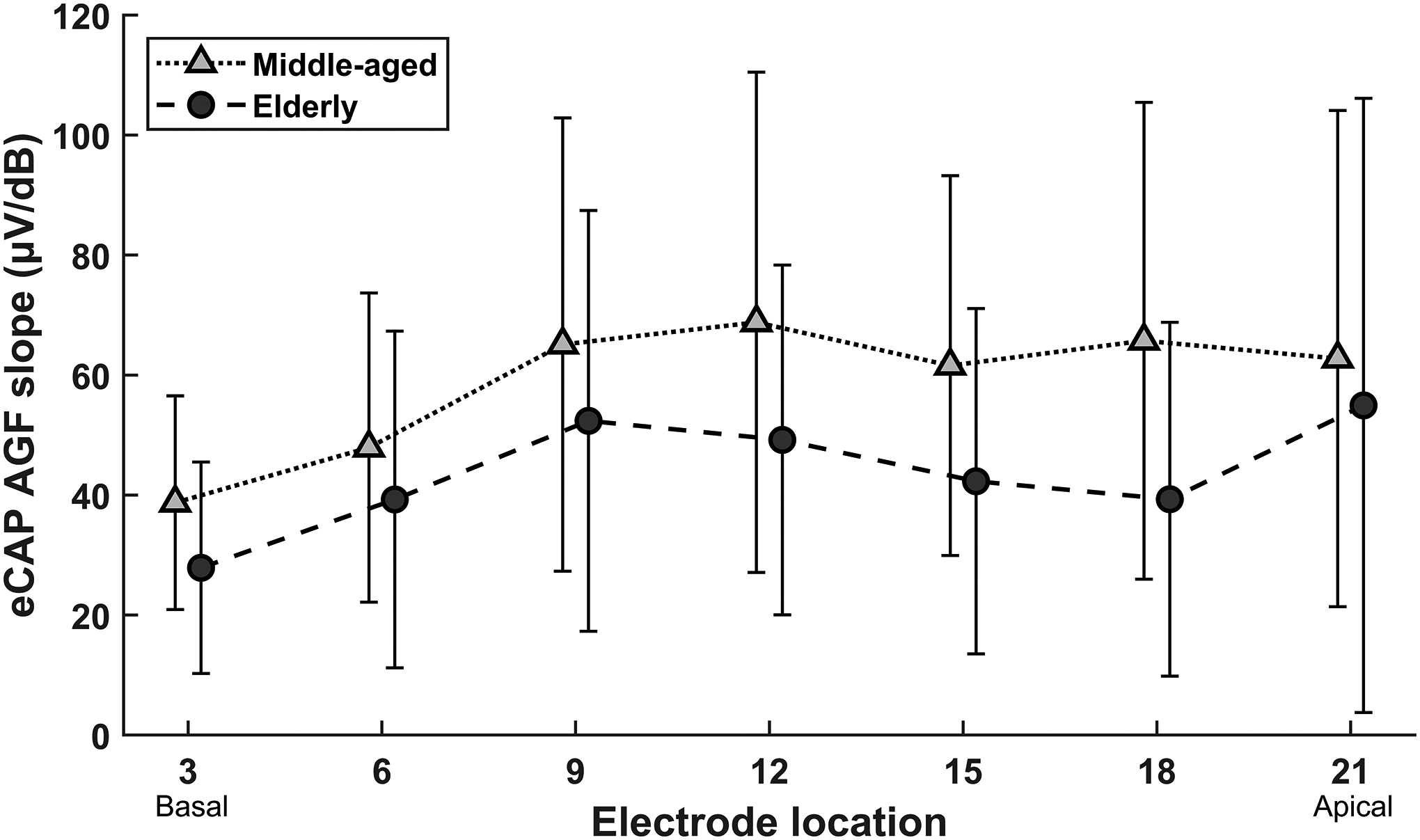
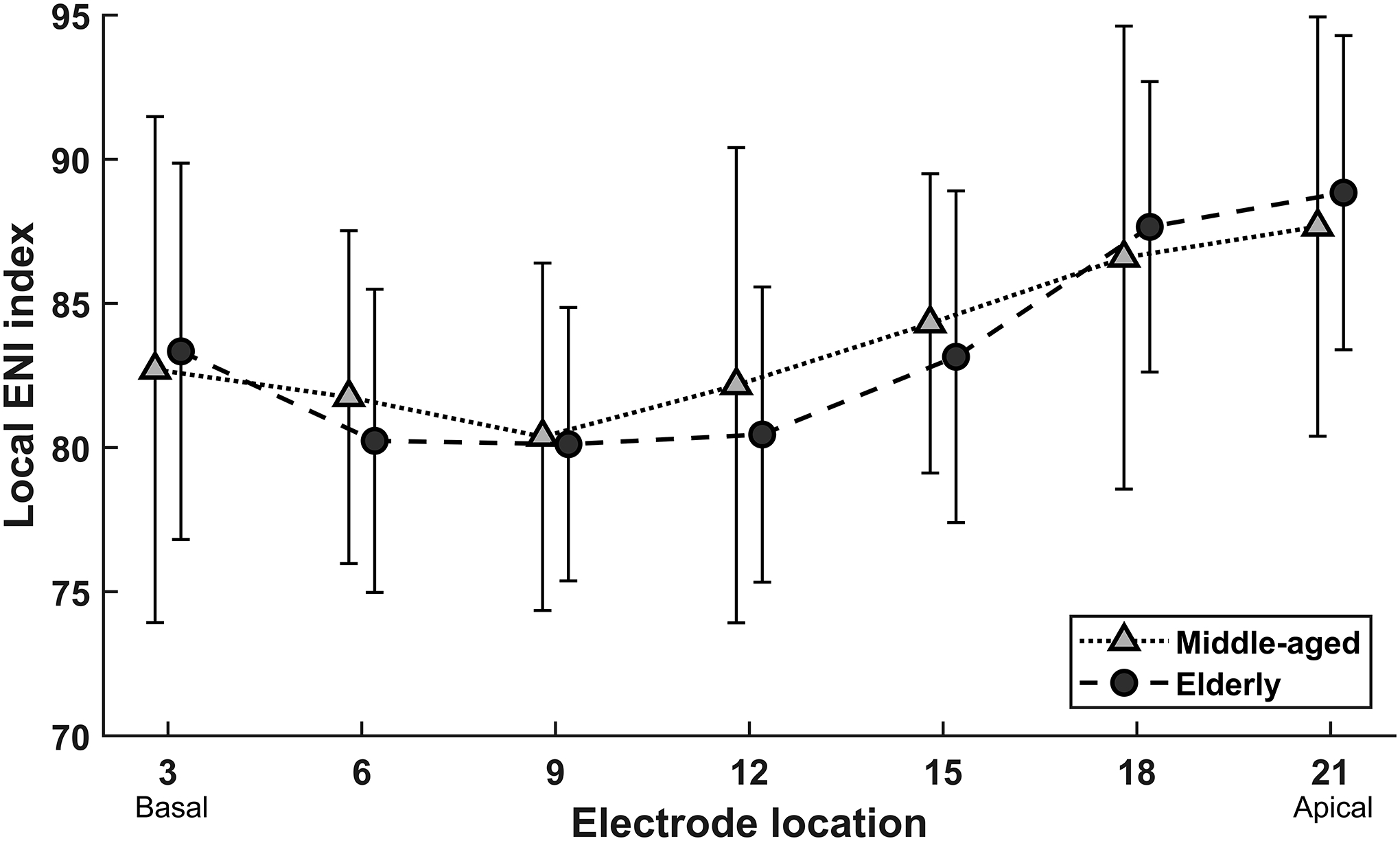
Design: Study participants included 40 postlingually deafened adult CI users. The participants were separated into two age groups based on age at testing in accordance with age classification terms used by the World Health Organization and the Medical Literature Analysis and Retrieval System Online bibliographic database. The middle-aged group included 16 participants between the ages of 45 and 64 years and the elderly group included 24 participants older than 65 years. Results were included from one ear for each participant. All participants used Cochlear Nucleus CIs in their test ears. For each participant, electrophysiological measures of the electrically evoked compound action potential (eCAP) were used to measure refractory recovery functions and amplitude growth functions (AGFs) at three to seven electrode sites across the electrode array. The eCAP parameters used in this study included the refractory recovery time estimated based on the eCAP refractory recovery function, the eCAP threshold, the slope of the eCAP AGF, and the negative-peak (i.e., N1) latency. The electrode-specific ENI was evaluated using an optimized combination of the eCAP parameters that represented the responsiveness of cochlear nerve fibers to electrical stimulation delivered by individual electrodes along the electrode array. The quality of the electrode-specific ENI was quantified by the local ENI index, a value between 0 and 100 where 0 and 100 represented the lowest- and the highest-quality ENI across all participants and electrodes in the study dataset, respectively.
Results: There were no significant age group differences in refractory times, eCAP thresholds, N1 latencies or local ENI indices. Slopes of the eCAP AGF were significantly larger in the middle-aged group compared to the elderly group. There was a significant effect of electrode location on each eCAP parameter, except for N1 latency. In addition, the local ENI index was significantly larger (i.e., better ENI) in the apical region than in the basal and middle regions of the cochlea for both age groups.
Conclusions: The model developed in this study can be used to estimate the quality of the ENI at individual electrode locations in CI users. The quality of the ENI is affected by the location of the electrode along the length of the cochlea. The method for estimating the quality of the ENI developed in this study holds promise for identifying electrodes with poor ENIs that could be deactivated from the clinical programming map. The ENI is not strongly affected by advanced age in middle-aged and elderly CI users.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures






Similar articles
-
Identifying Cochlear Implant Channels With Relatively Poor Electrode-Neuron Interfaces Using the Electrically Evoked Compound Action Potential.Ear Hear. 2020 Jul/Aug;41(4):961-973. doi: 10.1097/AUD.0000000000000844. Ear Hear. 2020. PMID: 31972772 Free PMC article.
-
The Relationship Between Cochlear Implant Speech Perception Outcomes and Electrophysiological Measures of the Electrically Evoked Compound Action Potential.Ear Hear. 2023 Nov-Dec 01;44(6):1485-1497. doi: 10.1097/AUD.0000000000001389. Epub 2023 May 17. Ear Hear. 2023. PMID: 37194125 Free PMC article.
-
Across-site patterns of electrically evoked compound action potential amplitude-growth functions in multichannel cochlear implant recipients and the effects of the interphase gap.Hear Res. 2016 Nov;341:50-65. doi: 10.1016/j.heares.2016.08.002. Epub 2016 Aug 10. Hear Res. 2016. PMID: 27521841 Free PMC article.
-
Effect of congenital inner ear malformations (IEMs) on electrically evoked compound action potential (ECAP) responses in cochlear implant children.Eur Arch Otorhinolaryngol. 2023 Dec;280(12):5193-5204. doi: 10.1007/s00405-023-08196-2. Epub 2023 Aug 22. Eur Arch Otorhinolaryngol. 2023. PMID: 37606729 Review.
-
The Panoramic ECAP Method: Estimating Patient-Specific Patterns of Current Spread and Neural Health in Cochlear Implant Users.J Assoc Res Otolaryngol. 2021 Oct;22(5):567-589. doi: 10.1007/s10162-021-00795-2. Epub 2021 Apr 23. J Assoc Res Otolaryngol. 2021. PMID: 33891218 Free PMC article. Review.
Cited by
-
A new method for removing artifacts from recordings of the electrically evoked compound action potential: Single-pulse stimulation.medRxiv [Preprint]. 2024 Jan 17:2024.01.17.24301435. doi: 10.1101/2024.01.17.24301435. medRxiv. 2024. PMID: 38293121 Free PMC article. Preprint.
-
Electrically evoked compound action potential polarity sensitivity, refractory-recovery, and behavioral multi-pulse integration as potential indices of neural health in cochlear-implant recipients.Hear Res. 2023 Jun;433:108764. doi: 10.1016/j.heares.2023.108764. Epub 2023 Apr 11. Hear Res. 2023. PMID: 37062161 Free PMC article. No abstract available.
-
Long-Term Auditory and Speech Outcomes of Cochlear Implantation in Children with IP-I Malformation.Laryngoscope. 2025 Jun;135(6):2120-2127. doi: 10.1002/lary.31988. Epub 2025 Jan 8. Laryngoscope. 2025. PMID: 39777670 Free PMC article.
-
Comparison of response properties of the electrically stimulated auditory nerve reported in human listeners and in animal models.Hear Res. 2022 Dec;426:108643. doi: 10.1016/j.heares.2022.108643. Epub 2022 Oct 28. Hear Res. 2022. PMID: 36343534 Free PMC article. Review.
References
-
- Abbas PJ, Hughes M, Brown CJ, et al. (2004). Channel Interaction in Cochlear Implant Users Evaluated Using the Electrically Evoked Compound Action Potential. Audiol Neurootol. 9. 203–213. - PubMed
-
- Birman CS, Powell HR, Gibson WP, et al. (2016). Cochlear implant outcomes in cochlea nerve aplasia and hypoplasia. Otol Neurotol, 37, 438–445. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
