

Differences in Cardiovascular Risk, Coronary Artery Disease, and Cardiac Events Between Black and White Individuals Enrolled in the PROMISE Trial
- PMID: 34935857
- PMCID: PMC8696694
- DOI: 10.1001/jamacardio.2021.5340
Differences in Cardiovascular Risk, Coronary Artery Disease, and Cardiac Events Between Black and White Individuals Enrolled in the PROMISE Trial
Abstract
Importance: Race and ethnicity have been studied as risk factors in cardiovascular disease. How risk factors, epicardial coronary artery disease, and cardiac events differ between Black and White individuals undergoing noninvasive testing for coronary artery disease is not known.
Objective: To assess differences in cardiovascular risk burden, coronary plaque, and major adverse cardiac events between Black and White individuals assigned to receive coronary computed tomography angiography (CCTA) or functional testing for stable chest pain.
Design, setting, and participants: A nested observational cohort study within the PROMISE trial was conducted at 193 outpatient sites in North America. A total of 1071 non-Hispanic Black (hereafter Black) and 7693 non-Hispanic White (hereafter White) participants with stable chest pain undergoing noninvasive cardiovascular testing were included. This analysis was conducted from February 13, 2015, to November 2, 2021.
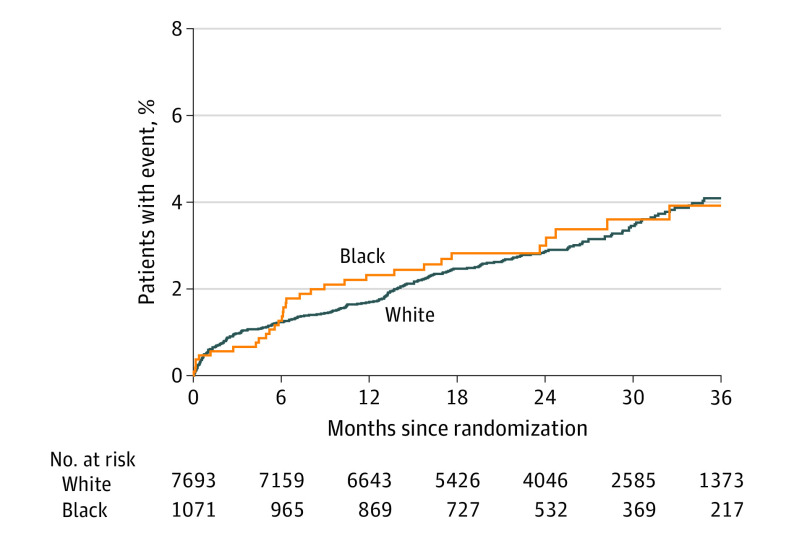
Main outcomes and measures: The primary end point was the composite of death, myocardial infarction, or hospitalization for unstable angina over a median follow-up of 24.4 months.
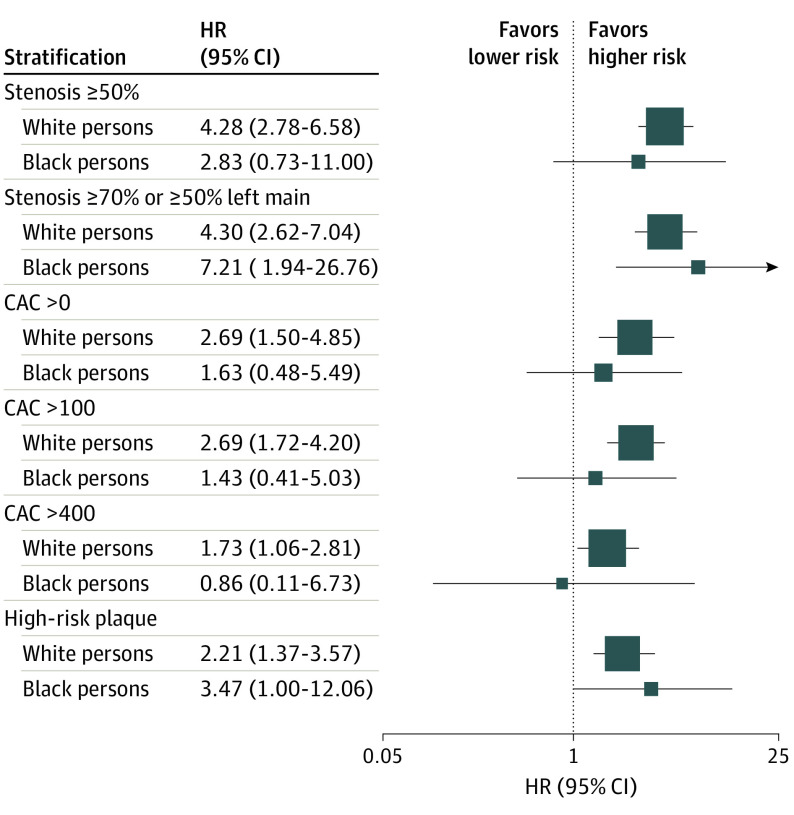
Results: Among 1071 Black individuals (12.2%) (women, 646 [60.3%]; mean [SD] age, 59 [8] years) and 7693 White individuals (87.8%) (women, 4029 [52.4%]; mean [SD] age, 61.1 [8.4] years), Black participants had a higher cardiovascular risk burden (more hypertension and diabetes), yet there was a similarly low major adverse cardiovascular events rate over a median 2-year follow-up (32 [3.0%] vs 243 [3.2%]; P = .84). Sensitivity analyses restricted to the 79.8% (6993 of 8764) individuals with a normal or mildly abnormal noninvasive testing result and the 54.3% (4559 of 8396) not receiving statin therapy yielded similar findings. In comparison of Black and White individuals in the CCTA group (n = 3323), significant coronary stenosis (hazard ratio [HR], 7.21; 95% CI, 1.94-26.76 vs HR, 4.30; 95% CI, 2.62-7.04) and high-risk plaque (HR, 3.47; 95% CI, 1.00-12.06 vs HR, 2.21; 95% CI, 1.37-3.57) were associated with major adverse cardiovascular events in both Black and White patients. However, with respect to epicardial coronary artery disease burden, Black individuals had a less-prevalent coronary artery calcium score greater than 0 (45.1% vs 63.2%; P < .001), coronary stenosis greater than or equal to 50% (32 [8.7%] vs 430 [14.6%]; P = .001), and high-risk plaque (139 [37.6%] vs 1547 [52.4%]; P < .001).
Conclusions and relevance: The findings of this study suggest that, despite a greater cardiovascular risk burden in Black persons, rates of coronary artery calcium, stenosis, and high-risk plaque observed via CCTA were lower in Black persons than White persons. This result suggests differences in cardiovascular risk burden and coronary plaque in Black and White individuals with stable chest pain.
Conflict of interest statement
Figures
References
-
- United States Census Bureau . ACS demographic and housing estimates: April 1, 2010, to July 1, 2018. Accessed February 13, 2015. https://factfinder.census.gov/faces/tableservices/jsf/pages/productview....
-
- Benjamin EJ, Muntner P, Alonso A, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56-e528. doi:10.1161/CIR.0000000000000659 - DOI - PubMed
-
- Gulati M, Levy PD, Mukherjee D, et al. . 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;2021:CIR0000000000001029. doi:10.1161/CIR.0000000000001029 - DOI - PubMed
-
- Voros S, Rinehart S, Qian Z, et al. . Prospective validation of standardized, 3-dimensional, quantitative coronary computed tomographic plaque measurements using radiofrequency backscatter intravascular ultrasound as reference standard in intermediate coronary arterial lesions: results from the ATLANTA (Assessment of Tissue Characteristics, Lesion Morphology, and Hemodynamics by Angiography With Fractional Flow Reserve, Intravascular Ultrasound and Virtual Histology, and Noninvasive Computed Tomography in Atherosclerotic Plaques) I study. JACC Cardiovasc Interv. 2011;4(2):198-208. doi:10.1016/j.jcin.2010.10.008 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
