

Metabolic Syndrome and Acute Respiratory Distress Syndrome in Hospitalized Patients With COVID-19
- PMID: 34935924
- PMCID: PMC8696573
- DOI: 10.1001/jamanetworkopen.2021.40568
Metabolic Syndrome and Acute Respiratory Distress Syndrome in Hospitalized Patients With COVID-19
Abstract
Importance: Obesity, diabetes, and hypertension are common comorbidities in patients with severe COVID-19, yet little is known about the risk of acute respiratory distress syndrome (ARDS) or death in patients with COVID-19 and metabolic syndrome.
Objective: To determine whether metabolic syndrome is associated with an increased risk of ARDS and death from COVID-19.
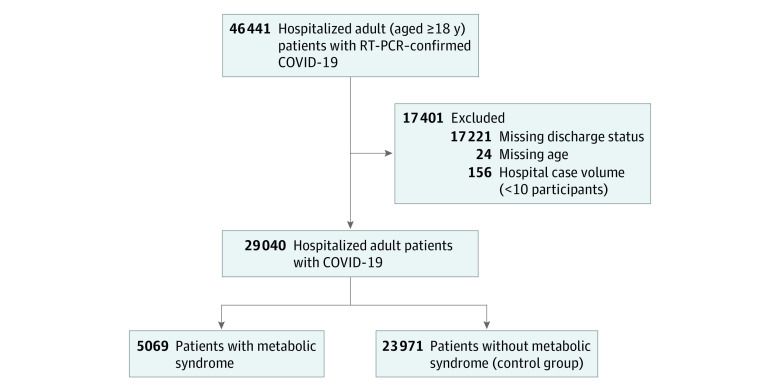
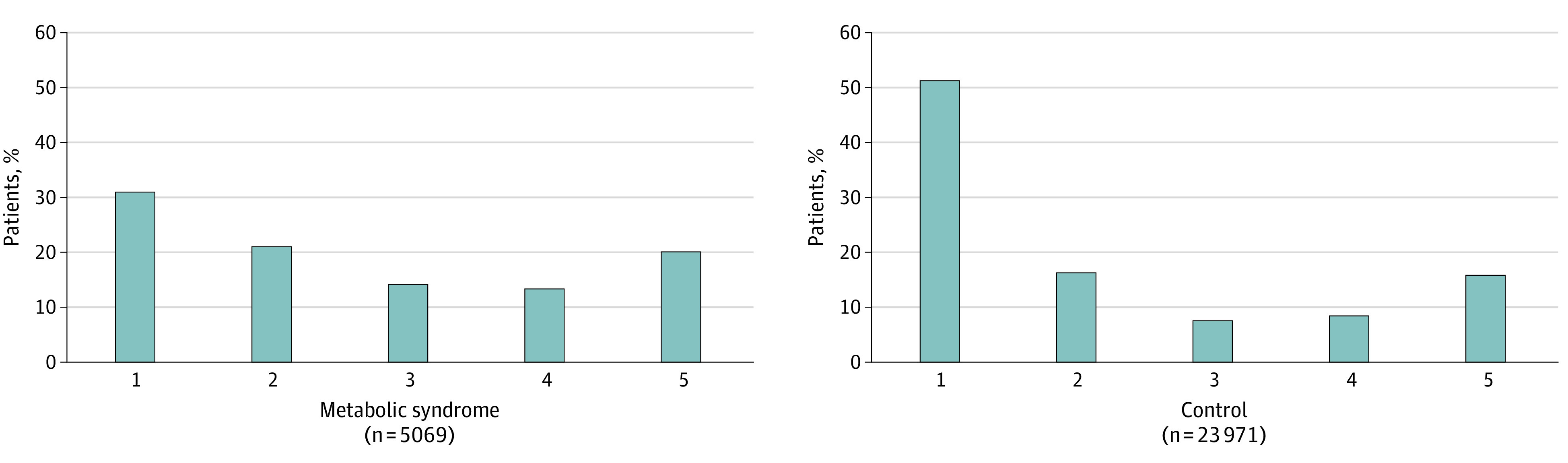
Design, setting, and participants: This multicenter cohort study used data from the Society of Critical Care Medicine Discovery Viral Respiratory Illness Universal Study collected from 181 hospitals across 26 countries from February 15, 2020, to February 18, 2021. Outcomes were compared between patients with metabolic syndrome (defined as ≥3 of the following criteria: obesity, prediabetes or diabetes, hypertension, and dyslipidemia) and a control population without metabolic syndrome. Participants included adult patients hospitalized for COVID-19 during the study period who had a completed discharge status. Data were analyzed from February 22 to October 5, 2021.
Exposures: Exposures were SARS-CoV-2 infection, metabolic syndrome, obesity, prediabetes or diabetes, hypertension, and/or dyslipidemia.
Main outcomes and measures: The primary outcome was in-hospital mortality. Secondary outcomes included ARDS, intensive care unit (ICU) admission, need for invasive mechanical ventilation, and length of stay (LOS).
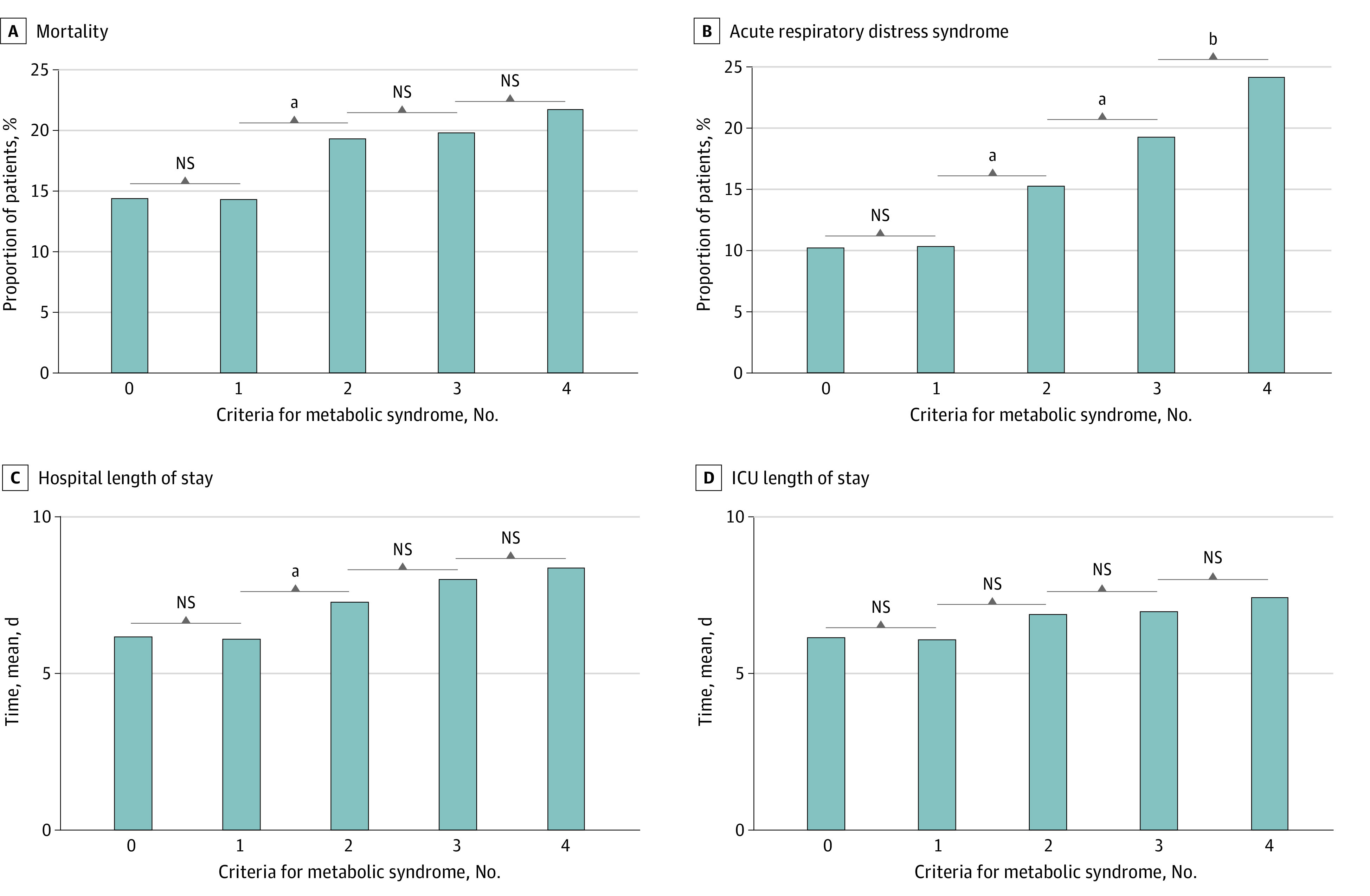
Results: Among 46 441 patients hospitalized with COVID-19, 29 040 patients (mean [SD] age, 61.2 [17.8] years; 13 059 [45.0%] women and 15713 [54.1%] men; 6797 Black patients [23.4%], 5325 Hispanic patients [18.3%], and 16 507 White patients [57.8%]) met inclusion criteria. A total of 5069 patients (17.5%) with metabolic syndrome were compared with 23 971 control patients (82.5%) without metabolic syndrome. In adjusted analyses, metabolic syndrome was associated with increased risk of ICU admission (adjusted odds ratio [aOR], 1.32 [95% CI, 1.14-1.53]), invasive mechanical ventilation (aOR, 1.45 [95% CI, 1.28-1.65]), ARDS (aOR, 1.36 [95% CI, 1.12-1.66]), and mortality (aOR, 1.19 [95% CI, 1.08-1.31]) and prolonged hospital LOS (median [IQR], 8.0 [4.2-15.8] days vs 6.8 [3.4-13.0] days; P < .001) and ICU LOS (median [IQR], 7.0 [2.8-15.0] days vs 6.4 [2.7-13.0] days; P < .001). Each additional metabolic syndrome criterion was associated with increased risk of ARDS in an additive fashion (1 criterion: 1147 patients with ARDS [10.4%]; P = .83; 2 criteria: 1191 patients with ARDS [15.3%]; P < .001; 3 criteria: 817 patients with ARDS [19.3%]; P < .001; 4 criteria: 203 patients with ARDS [24.3%]; P < .001).
Conclusions and relevance: These findings suggest that metabolic syndrome was associated with increased risks of ARDS and death in patients hospitalized with COVID-19. The association with ARDS was cumulative for each metabolic syndrome criteria present.
Conflict of interest statement
Figures
References
-
- Domecq JP, Lal A, Sheldrick CR, et al. ; Society of Critical Care Medicine Discovery Viral Infection and Respiratory Illness Universal Study (VIRUS): COVID-19 Registry Investigator Group . Outcomes of patients with coronavirus disease 2019 receiving organ support therapies: the International Viral Infection and Respiratory Illness Universal Study Registry. Crit Care Med. 2021;49(3):437-448. doi: 10.1097/CCM.0000000000004879 - DOI - PMC - PubMed
-
- Richardson S, Hirsch JS, Narasimhan M, et al. ; the Northwell COVID-19 Research Consortium . Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052-2059. doi: 10.1001/jama.2020.6775 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
