

Tracheostomy in COVID-19 acute respiratory distress syndrome patients and follow-up: A parisian bicentric retrospective cohort
- PMID: 34936655
- PMCID: PMC8694414
- DOI: 10.1371/journal.pone.0261024
Tracheostomy in COVID-19 acute respiratory distress syndrome patients and follow-up: A parisian bicentric retrospective cohort
Abstract
Background: Tracheostomy has been proposed as an option to help organize the healthcare system to face the unprecedented number of patients hospitalized for a COVID-19-related acute respiratory distress syndrome (ARDS) in intensive care units (ICU). It is, however, considered a particularly high-risk procedure for contamination. This paper aims to provide our experience in performing tracheostomies on COVID-19 critically ill patients during the pandemic and its long-term local complications.
Methods: We performed a retrospective analysis of prospectively collected data of patients tracheostomized for a COVID-19-related ARDS in two university hospitals in the Paris region between January 27th (date of first COVID-19 admission) and May 18th, 2020 (date of last tracheostomy performed). We focused on tracheostomy technique (percutaneous versus surgical), timing (early versus late) and late complications.
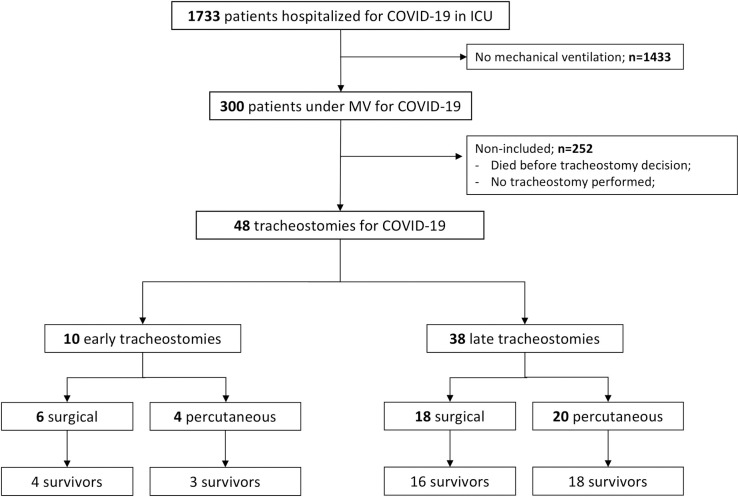
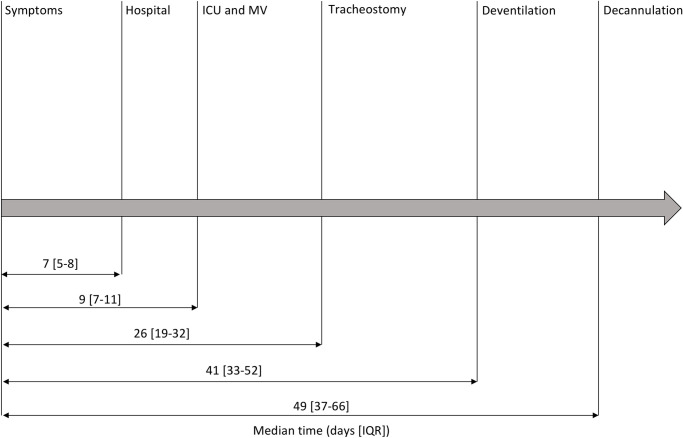
Results: Forty-eight tracheostomies were performed with an equal division between surgical and percutaneous techniques. There was no difference in patients' characteristics between surgical and percutaneous groups. Tracheostomy was performed after a median of 17 [12-22] days of mechanical ventilation (MV), with 10 patients in the "early" group (≤ day 10) and 38 patients in the "late" group (> day 10). Survivors required MV for a median of 32 [22-41] days and were ultimately decannulated with a median of 21 [15-34] days spent on cannula. Patients in the early group had shorter ICU and hospital stays (respectively 15 [12-19] versus 35 [25-47] days; p = 0.002, and 21 [16-28] versus 54 [35-72] days; p = 0.002) and spent less time on MV (respectively 17 [14-20] and 35 [27-43] days; p<0.001). Interestingly, patients in the percutaneous group had shorter hospital and rehabilitation center stays (respectively 44 [34-81] versus 92 [61-118] days; p = 0.012, and 24 [11-38] versus 45 [22-71] days; p = 0.045). Of the 30 (67%) patients examined by a head and neck surgeon, 17 (57%) had complications with unilateral laryngeal palsy (n = 5) being the most prevalent.
Conclusions: Tracheostomy seems to be a safe procedure that could help ICU organization by delegating work to a separate team and favoring patient turnover by allowing faster transfer to step-down units. Following guidelines alone was found sufficient to prevent the risk of aerosolization and contamination of healthcare professionals.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Durbin CG. Tracheostomy: Why, When, and How? Respir Care. 2010. Aug 1;55(8):1056–68. - PubMed
-
- Constantin J-M, Maury E, Aubrun F. Rapport SFAR: Preconisations-pour-lutilisation-parcimonieuse-des-molecules-en-tension-durant-la-pandemie-covid-19. 2020. Apr. Available from: https://sfar.org/download/preconisations-pour-lutilisation-parcimonieuse... = 26081&refresh = 5ea1be84aec4f1587658372
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
