

Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients
- PMID: 34937145
- PMCID: PMC8757570
- DOI: 10.1056/NEJMoa2116846
Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients
Abstract
Background: Remdesivir improves clinical outcomes in patients hospitalized with moderate-to-severe coronavirus disease 2019 (Covid-19). Whether the use of remdesivir in symptomatic, nonhospitalized patients with Covid-19 who are at high risk for disease progression prevents hospitalization is uncertain.
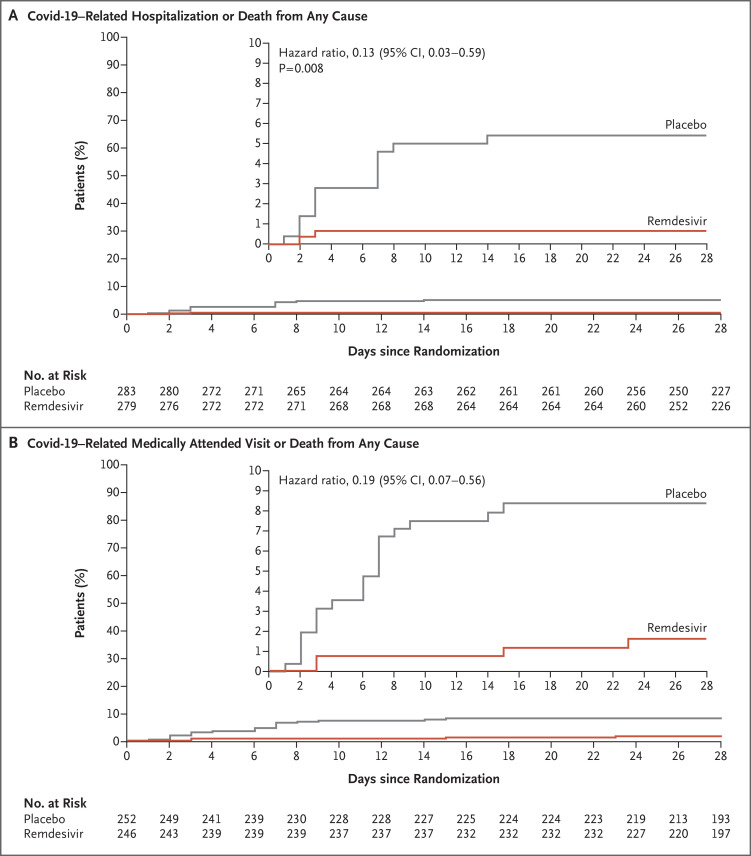
Methods: We conducted a randomized, double-blind, placebo-controlled trial involving nonhospitalized patients with Covid-19 who had symptom onset within the previous 7 days and who had at least one risk factor for disease progression (age ≥60 years, obesity, or certain coexisting medical conditions). Patients were randomly assigned to receive intravenous remdesivir (200 mg on day 1 and 100 mg on days 2 and 3) or placebo. The primary efficacy end point was a composite of Covid-19-related hospitalization or death from any cause by day 28. The primary safety end point was any adverse event. A secondary end point was a composite of a Covid-19-related medically attended visit or death from any cause by day 28.
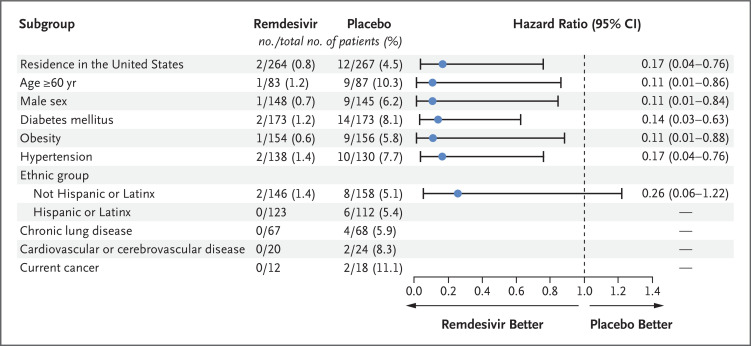
Results: A total of 562 patients who underwent randomization and received at least one dose of remdesivir or placebo were included in the analyses: 279 patients in the remdesivir group and 283 in the placebo group. The mean age was 50 years, 47.9% of the patients were women, and 41.8% were Hispanic or Latinx. The most common coexisting conditions were diabetes mellitus (61.6%), obesity (55.2%), and hypertension (47.7%). Covid-19-related hospitalization or death from any cause occurred in 2 patients (0.7%) in the remdesivir group and in 15 (5.3%) in the placebo group (hazard ratio, 0.13; 95% confidence interval [CI], 0.03 to 0.59; P = 0.008). A total of 4 of 246 patients (1.6%) in the remdesivir group and 21 of 252 (8.3%) in the placebo group had a Covid-19-related medically attended visit by day 28 (hazard ratio, 0.19; 95% CI, 0.07 to 0.56). No patients had died by day 28. Adverse events occurred in 42.3% of the patients in the remdesivir group and in 46.3% of those in the placebo group.
Conclusions: Among nonhospitalized patients who were at high risk for Covid-19 progression, a 3-day course of remdesivir had an acceptable safety profile and resulted in an 87% lower risk of hospitalization or death than placebo. (Funded by Gilead Sciences; PINETREE ClinicalTrials.gov number, NCT04501952; EudraCT number, 2020-003510-12.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
The Goldilocks Time for Remdesivir - Is Any Indication Just Right?N Engl J Med. 2022 Jan 27;386(4):385-387. doi: 10.1056/NEJMe2118579. Epub 2021 Dec 22. N Engl J Med. 2022. PMID: 34936760 Free PMC article. No abstract available.
-
Outpatient Remdesivir to Prevent Progression to Severe Covid-19.N Engl J Med. 2022 Mar 17;386(11):1094. doi: 10.1056/NEJMc2200591. Epub 2022 Feb 16. N Engl J Med. 2022. PMID: 35172052 No abstract available.
-
In high-risk outpatients with COVID-19, remdesivir reduced COVID-19-related hospitalization or all-cause death at 28 d.Ann Intern Med. 2022 May;175(5):JC50. doi: 10.7326/J22-0026. Epub 2022 May 3. Ann Intern Med. 2022. PMID: 35500263
-
Remdesivir senkt Covid-Hospitalisierungsrate.MMW Fortschr Med. 2022 Jun;164(11):28. doi: 10.1007/s15006-022-1234-z. MMW Fortschr Med. 2022. PMID: 35650486 Free PMC article. German. No abstract available.
References
-
- WHO Director-General’s opening remarks at the media briefing on COVID-19. Geneva: World Health Organization, March 11, 2020. (https://www.who.int/director-general/speeches/detail/who-director-genera...).
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical