

Interstitial pneumonia with autoimmune features: challenges and controversies
- PMID: 34937706
- PMCID: PMC9488577
- DOI: 10.1183/16000617.0177-2021
Interstitial pneumonia with autoimmune features: challenges and controversies
Abstract
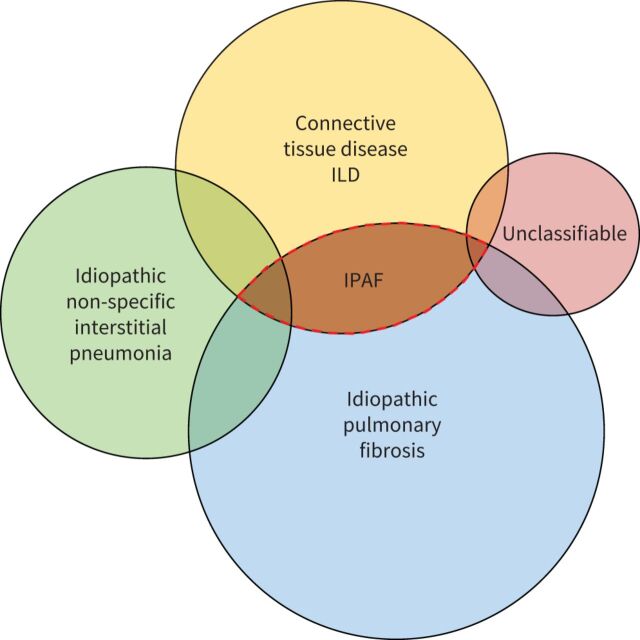
The presence of clinical, serological and/or radiological features suggestive, but not confirmatory, of a defined connective tissue disease in patients with interstitial lung disease is a relatively frequent occurrence. In 2015, the European Respiratory Society and the American Thoracic Society proposed classification criteria for the interstitial pneumonia with autoimmune features (IPAF) research entity to capture such patients in a standardised manner, with the intention of nurturing clinical research. This initiative resulted in the publication of several series of IPAF patients, with significant variation between cohorts in clinical characteristics, outcome and the application of IPAF criteria in patient selection. From this increasing body of published work, it has become apparent that revision of IPAF criteria is now required in order to justify the eventual designation of IPAF as a standalone diagnostic term, as opposed to a provisional entity put forward as a basis for clinical research. This review covers the current state of IPAF, conclusions that can and cannot be drawn from the IPAF evidence base, and ongoing uncertainties that require further expert group consideration.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: J.A. Mackintosh has nothing to disclose. Conflict of interest: A.U. Wells reports personal fees from Roche, Boehringer Ingelheim and Bayer outside the submitted work. Conflict of interest: V. Cottin reports personal fees and non-financial support from Actelion; grants, personal fees and non-financial support from Boehringer Ingelheim; personal fees from Bayer/MSD; personal fees and non-financial support from Roche/Promedior; and personal fees from Sanofi, Celgene/BMS, Galapagos, Galecto, Shionogi, AstraZeneca, Fibrogen, RedX and PureTech, outside the submitted work. Conflict of interest: A.G. Nicholson reports consulting fees received from Galapagos, Boehringer Ingelheim, Roche and Medical Quantitative Image Analysis in relation to idiopathic pulmonary fibrosis, outside the submitted work; and payment for educational activities in relation to ILD outside the submitted work. Conflict of interest: E.A. Renzoni reports receiving grants or contracts from Boehringer Ingelheim outside the submitted work; lecture fees paid to the institution from Boehringer Ingelheim, Roche and Chiesi outside the submitted work; and support for attending ATS conference from Boehringer Ingelheim outside the submitted work.
Figures

Comment in
-
Some take-home messages from the 9th International Meeting on Pulmonary Rare Diseases and Orphan Drugs.Eur Respir Rev. 2021 Dec 22;30(162):210258. doi: 10.1183/16000617.0258-2021. Print 2021 Dec 31. Eur Respir Rev. 2021. PMID: 34937707 Free PMC article.
References
-
- Lundberg IE, Tjärnlund A, Bottai M, et al. . 2017. European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Arthritis Rheum 2017; 69: 2271–2282. doi:10.1002/art.40320 - DOI - PMC - PubMed
-
- Shiboski CH, Shiboski SC, Seror R, et al. . 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren's Syndrome: a consensus and data-driven methodology involving three international patient cohorts. Arthritis Rheum 2017; 69: 35–45. doi:10.1002/art.39859 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical