

Neutralization of SARS-CoV-2 Variants of Concern in Kidney Transplant Recipients after Standard COVID-19 Vaccination
- PMID: 34937771
- PMCID: PMC8763153
- DOI: 10.2215/CJN.11820921
Neutralization of SARS-CoV-2 Variants of Concern in Kidney Transplant Recipients after Standard COVID-19 Vaccination
Abstract
Background and objectives: Antibody response after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccination is impaired in kidney transplant recipients. Emerging variants, such as B.1.617.2 (δ), are of particular concern because of their higher transmissibility and partial immune escape. Little is known about protection against these variants in immunocompromised patients.
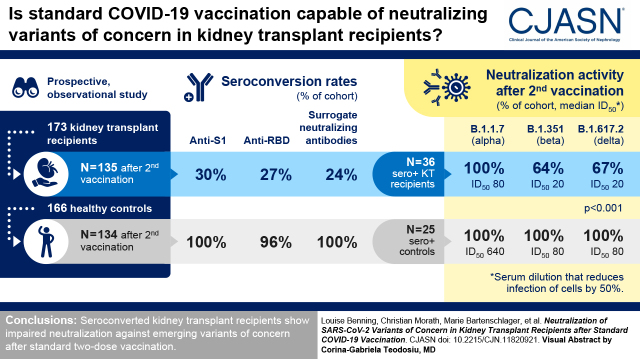
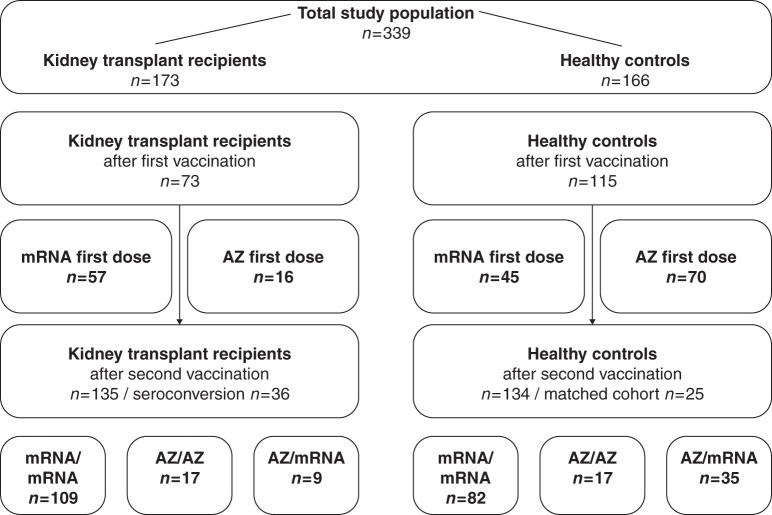
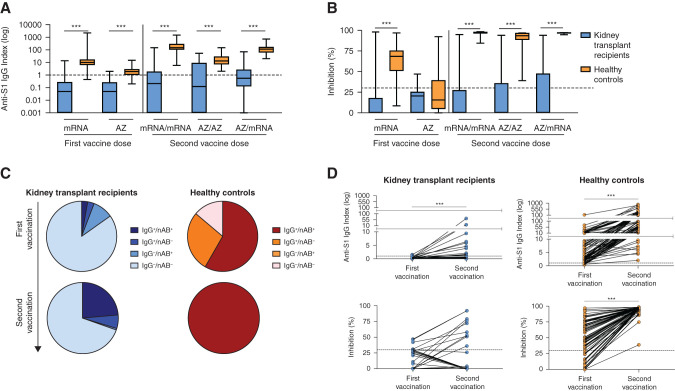
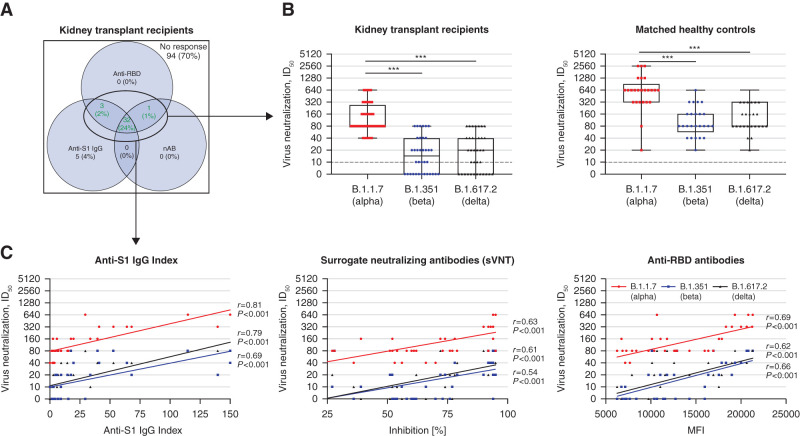
Design, setting, participants, & measurements: In this prospective two-center study, antispike 1 IgG and surrogate neutralizing antibodies were measured in 173 kidney transplant recipients and 166 healthy controls with different vaccination schedules. In addition, different SARS-CoV-2 epitope antibodies from 135 vaccinated kidney transplant recipients were compared with antibodies in 25 matched healthy controls after second vaccination. In 36 kidney transplant recipients with seroconversion, neutralization against B.1.1.7 (α), B.1.351 (β), and B.1.617.2 (δ) was determined on VeroE6 cells and compared with neutralization in 25 healthy controls.
Results: Kidney transplant recipients had significantly lower seroconversion rates compared with healthy controls. After the second vaccination, antispike 1, antireceptor-binding domain, and surrogate neutralizing antibodies were detectable in 30%, 27%, and 24% of kidney transplant recipients, respectively. This compares with 100%, 96%, and 100% in healthy controls, respectively (P<0.001). Neutralization against B.1.1.7 was detectable in all kidney transplant recipients with seroconversion, with a median serum dilution that reduces infection of cells by 50% of 80 (interquartile range, 80-320). In contrast, only 23 of 36 (64%) and 24 of 36 (67%) kidney transplant recipients showed neutralization against B.1.351 and B.1.617.2, respectively, with median serum dilutions that reduce infection of cells by 50% of 20 (interquartile range, 0-40) and 20 (interquartile range, 0-40), respectively. Neutralization against different variants was significantly higher in healthy controls (P<0.001), with all patients showing neutralization against all tested variants.
Conclusions: Seroconverted kidney transplant recipients show impaired neutralization against emerging variants of concern after standard two-dose vaccination.
Clinical trial registry name and registration number: Observational study to assess the SARS-CoV-2 specific immune response in kidney transplant recipients (COVID-19 related immune response), DRKS00024668.
Keywords: COVID-19; SARS-CoV-2; kidney transplantation; vaccination; variants of concern.
Copyright © 2022 by the American Society of Nephrology.
Figures
Comment in
-
Protection against SARS-CoV-2 Variants with COVID-19 Vaccination in Kidney Transplant Recipients.Clin J Am Soc Nephrol. 2022 Jan;17(1):3-5. doi: 10.2215/CJN.14881121. Epub 2021 Dec 22. Clin J Am Soc Nephrol. 2022. PMID: 34937770 Free PMC article. No abstract available.
References
-
- Hilbrands LB, Duivenvoorden R, Vart P, Franssen CFM, Hemmelder MH, Jager KJ, Kieneker LM, Noordzij M, Pena MJ, Vries H, Arroyo D, Covic A, Crespo M, Goffin E, Islam M, Massy ZA, Montero N, Oliveira JP, Roca Muñoz A, Sanchez JE, Sridharan S, Winzeler R, Gansevoort RT; ERACODA Collaborators : COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol Dial Transplant 35: 1973–1983, 2020 - PMC - PubMed
-
- Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, Curtis HJ, Mehrkar A, Evans D, Inglesby P, Cockburn J, McDonald HI, MacKenna B, Tomlinson L, Douglas IJ, Rentsch CT, Mathur R, Wong AYS, Grieve R, Harrison D, Forbes H, Schultze A, Croker R, Parry J, Hester F, Harper S, Perera R, Evans SJW, Smeeth L, Goldacre B: Factors associated with COVID-19-related death using OpenSAFELY. Nature 584: 430–436, 2020 - PMC - PubMed
-
- Bertrand D, Hamzaoui M, Lemée V, Lamulle J, Hanoy M, Laurent C, Lebourg L, Etienne I, Lemoine M, Le Roy F, Nezam D, Plantier JC, Boyer O, Guerrot D, Candon S: Antibody and T cell response to SARS-CoV-2 messenger RNA BNT162b2 vaccine in kidney transplant recipients and hemodialysis patients. J Am Soc Nephrol 32: 2147–2152, 2021 - PMC - PubMed
-
- Danthu C, Hantz S, Dahlem A, Duval M, Ba B, Guibbert M, El Ouafi Z, Ponsard S, Berrahal I, Achard JM, Bocquentin F, Allot V, Rerolle JP, Alain S, Touré F: Humoral response after SARS-CoV-2 mRNA vaccination in a cohort of hemodialysis patients and kidney transplant recipients. J Am Soc Nephrol 32: 2153–2158, 2021 - PMC - PubMed
-
- Sattler A, Schrezenmeier E, Weber UA, Potekhin A, Bachmann F, Straub-Hohenbleicher H, Budde K, Storz E, Proß V, Bergmann Y, Thole LM, Tizian C, Hölsken O, Diefenbach A, Schrezenmeier H, Jahrsdörfer B, Zemojtel T, Jechow K, Conrad C, Lukassen S, Stauch D, Lachmann N, Choi M, Halleck F, Kotsch K: Impaired humoral and cellular immunity after SARS-CoV-2 BNT162b2 (tozinameran) prime-boost vaccination in kidney transplant recipients. J Clin Invest 131: 150175, 2021 - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
