

Buccal periosteal inversion (BUPI) for defect closure and keratinized gingiva width preservation after tooth extraction - technique modification
- PMID: 34938049
- PMCID: PMC8665163
- DOI: 10.1016/j.sdentj.2021.05.004
Buccal periosteal inversion (BUPI) for defect closure and keratinized gingiva width preservation after tooth extraction - technique modification
Abstract
Introduction: Several techniques and methods have been proposed to cover alveolar bone after tooth extraction when soft tissue is lacking. Some authors recommend soft tissue flap techniques, and others advocate different types of materials for socket covering. In this article, the authors use a modified buccal inversion technique for adequate coverage of the alveolar ridge to ensure its preservation and to minimize soft tissue shrinkage and loss of keratinized gingiva after tooth extraction. This local mucogingival-periosteal plastic procedure was named by the authors the "Buccal Periosteal Inversion technique" or simply BUPI.
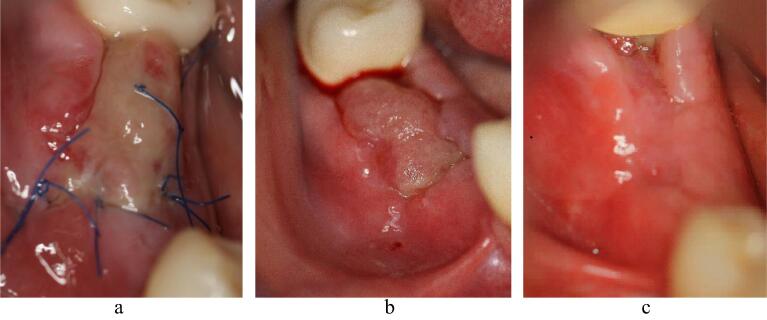
Materials and methods: After extraction of a fractured, endodontically compromised lower right first molar, the BUPI technique was performed to cover the alveolus. After reflecting the two-sided full-thickness flap, the periosteum was split in the cranial direction. The inverted periosteum is used to provide tension-free defect closure of the postextractional defect. Detailed technique implementation and patient postoperative healing are presented here in detail.
Results: Postoperative evaluation at six weeks was presented with photos showing adequate surgical site healing, no signs of infection or dehiscence, and no crestal shift of the keratinized gingiva.
Conclusion: The buccal periosteal inversion (BUPI) technique is a modified technique that allows full socket coverage, avoiding a keratinized gingiva shift in the crestal direction using only the periosteum as a cover material. By inverting the buccal ridge periosteum alone from its normal position, the osteoclastic effect on the buccal bony wall will be eliminated, and this procedure abolishes the need for additional alveolar coverage materials.
Keywords: Alveolar protection; Buccal ridge preservation; Periosteal inversion; Periosteum; Periosteum inversion.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



Similar articles
-
Inverted periosteal flap: an alternative to the buccal advancement flap for tension-free, watertight closure.J Oral Maxillofac Surg. 2014 Jul;72(7):1244-50. doi: 10.1016/j.joms.2014.03.006. Epub 2014 Mar 20. J Oral Maxillofac Surg. 2014. PMID: 24768423
-
[Dental implantation and soft tissue augmentation after ridge preservation in a molar site: a case report].Beijing Da Xue Xue Bao Yi Xue Ban. 2016 Dec 18;48(6):1090-1094. Beijing Da Xue Xue Bao Yi Xue Ban. 2016. PMID: 27987520 Chinese.
-
Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing.Clin Oral Implants Res. 2013 Nov;24(11):1231-7. doi: 10.1111/j.1600-0501.2012.02535.x. Epub 2012 Jul 12. Clin Oral Implants Res. 2013. PMID: 22784417 Clinical Trial.
-
Flapless alveolar ridge preservation utilizing the "socket-plug" technique: clinical technique and review of the literature.J Oral Implantol. 2014 Dec;40(6):690-8. doi: 10.1563/AAID-JOI-D-12-00028. J Oral Implantol. 2014. PMID: 25506661 Review.
-
Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis.J Clin Periodontol. 2019 Jun;46 Suppl 21:195-223. doi: 10.1111/jcpe.13057. J Clin Periodontol. 2019. PMID: 30623987
References
-
- Barone A., Toti P., Piattelli A., et al. Extraction socket healing in humans after ridge preservation techniques: comparison between flapless and flapped procedures in a randomized clinical trial. J. Periodontol. 2014;85(1):14–23. doi: 10.1902/jop.2013.120711. Epub 2013 May 20 PubMed PMID: 23688103. - DOI - PubMed
-
- Bassir SH, Alhareky M, Wangsrimongkol B, et al. Systematic Review and Meta-Analysis of Hard Tissue Outcomes of Alveolar Ridge Preservation. Int. J. Oral Maxillofac Implants. 2018 Sep/Oct;33(5):979-994. doi: 10.11607/jomi.6399. Review. PubMed PMID: 30231083. - PubMed
LinkOut - more resources
Full Text Sources
