

Ultrasound Features of Adhesive Capsulitis
- PMID: 34940958
- PMCID: PMC8696249
- DOI: 10.1007/s40744-021-00413-w
Ultrasound Features of Adhesive Capsulitis
Abstract
Introduction: Adhesive capsulitis (AC), which is characterised by shoulder pain and a limited range of motion (ROM), is usually diagnosed on the basis of clinical suspicion, with imaging only being used to exclude other causes of similar symptoms. The aim of this study was to identify and describe the typical ultrasound (US) features of AC in a group of patients with shoulder pain and stiffness.
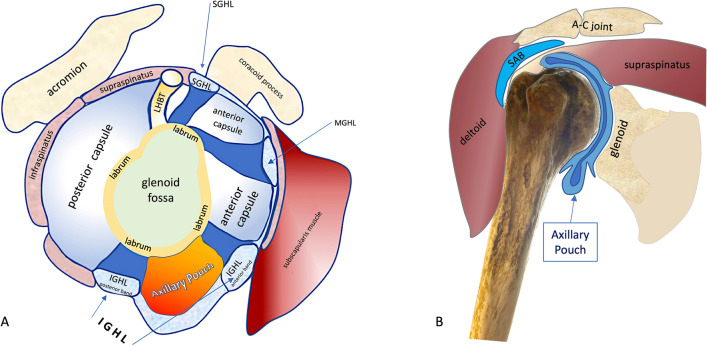
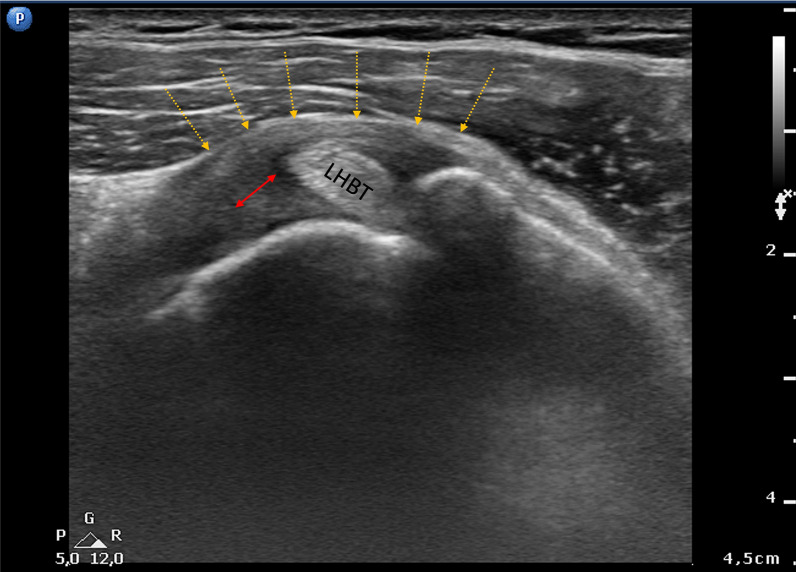
Methods: This was a cross-sectional study of 1486 patients with AC in which two experienced US specialists examined the axillary pouch (AP), the coracohumeral ligament (CHL), the superior glenohumeral ligament (SGHL), and the long head of the biceps tendon (LHBT), and dynamically visualised the infraspinatus tendon during passive external rotation (PER) during a US evaluation of shoulder ROM.
Results: AC was confirmed in 106 patients (7.1%). Thickening of the AP of more than 4 mm was observed in 93.4% of the patients, whereas 6.6% showed AP thickening of less than 4 mm but more than 60% of the thickening in the contralateral shoulder. Effusion within the LHBT sheath was detected in 71% of the patients, and thickening of the CHL or SGHL in 88%. The dynamic study of the infraspinatus tendon showed reduced sliding with folding towards the joint capsule in 73% of cases, thus changing the tendon's profile from flat to concave during PER. The reduced tendon sliding was associated with a bouncing movement that returned the tendon to its baseline resting position in 41.5% of cases.
Conclusions: We believe a sufficiently experienced US specialist can confirm a clinical diagnosis of AC by carrying out a comparative study of APs, evaluating the thickness of the CHL and SGHL, and detecting reduced sliding of the infraspinatus tendon.
Keywords: Adhesive capsulitis; Axillary pouch; Coracohumeral ligament; Frozen shoulder; Ultrasound.
© 2021. The Author(s).
Figures






References
-
- Duplay ES. De la peri-arthrite scapulo humerale et des raideurs de l’epaule qui en son la consequence. Arch Gen Med. 1872;20:31–42.
-
- Codman E. The shoulder: rupture of the supraspinatus tendon and other lesions in or about the subcromial bursa. Boston: Todd; 1934.
-
- Neviaser JS. Adhesive capsulitis of the shoulder: a study of the pathological findings in periarthritis of the shoulder. J Am Acad Orthop Surg. 1945;27:211–222.
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
