

Pulmonary Vasculitides: A Radiological Review Emphasizing Parenchymal HRCT Features
- PMID: 34943555
- PMCID: PMC8700038
- DOI: 10.3390/diagnostics11122318
Pulmonary Vasculitides: A Radiological Review Emphasizing Parenchymal HRCT Features
Abstract
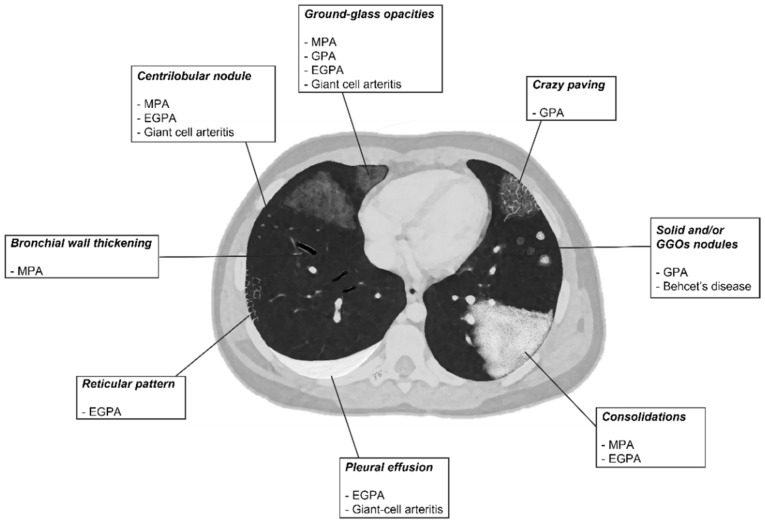
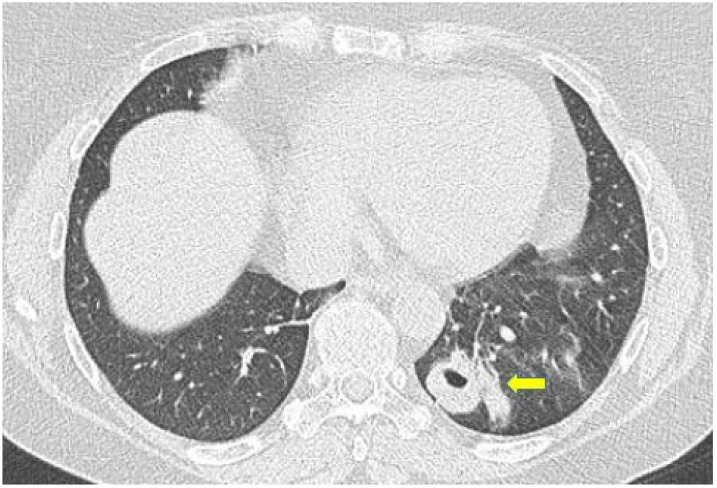
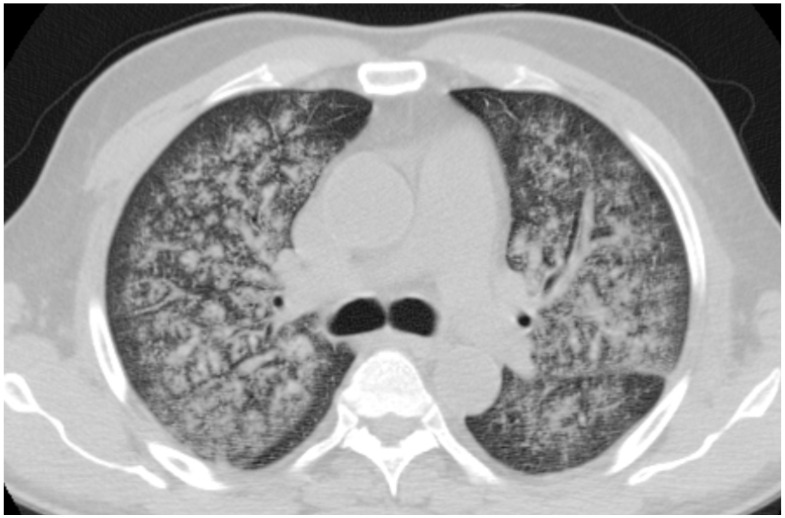
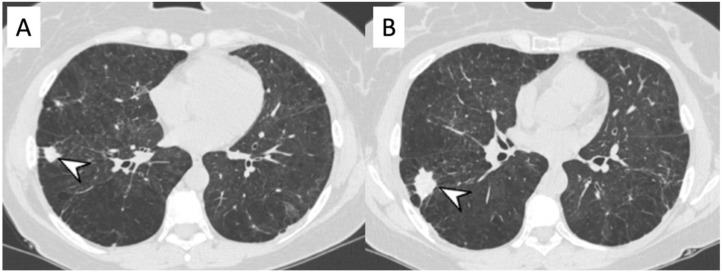
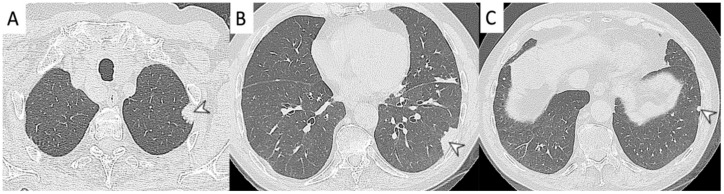
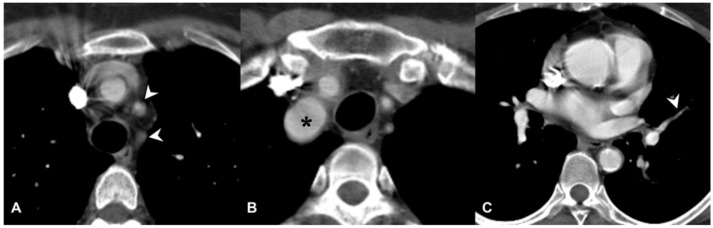
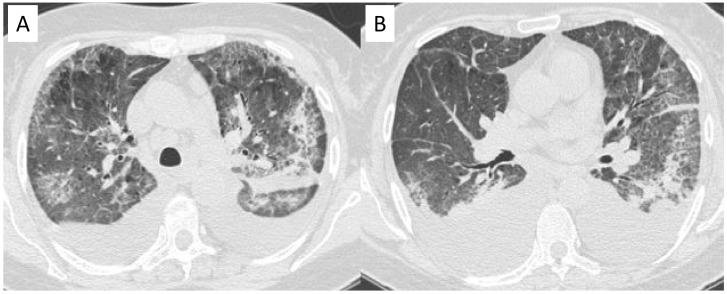
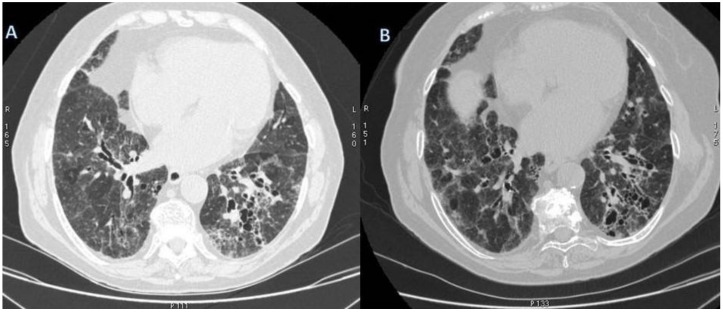
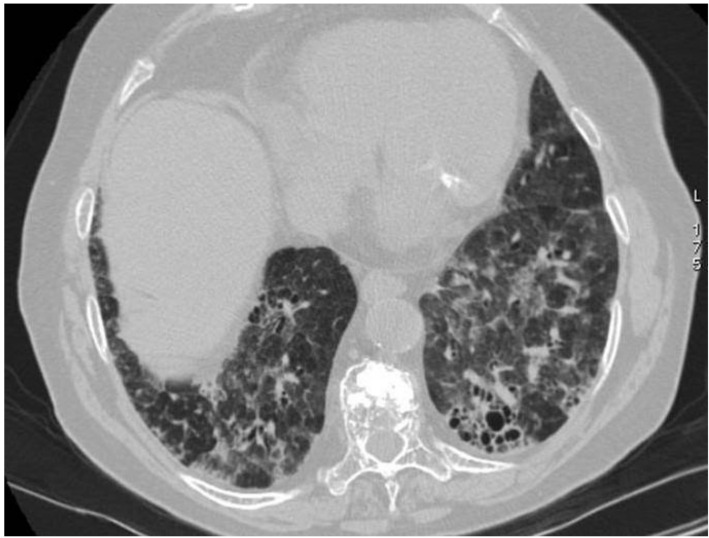
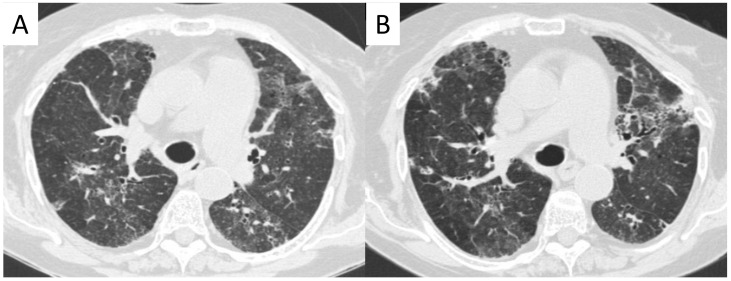
Vasculitides represent a heterogeneous group of immune-mediated disorders, characterized by a systemic inflammatory destructive process of the blood vessels resulting either in ischemia or hemorrhage. The organ involved and vessel size influence the pattern of presentation of the pathology. The lung is commonly involved in systemic vasculitides, with heterogeneous clinical, radiological, and histopathological presentations. Primary vasculitides most commonly associated with lung parenchymal involvement include small-vessel antineutrophil cytoplasmic autoantibody (ANCA)-associated vasculitides, such as granulomatosis with polyangiitis (GPA), eosinophilic granulomatosis with polyangiitis (EGPA), and microscopic polyangiitis (MPA). Several studies have reported cases of interstitial lung diseases (ILDs) associated with systemic vasculitis, particularly those positive for ANCA associated vasculitis/vasculitidis: AAV. We have selected from our case series different radiological features of pulmonary vasculitis (i.e., solitary or multiple nodules, cavitary lesions, nodules with centrilobular or peribronchial distribution, airspace consolidations, "crazy paving" appearance, interstitial disease), including cases with interstitial lung alterations. Therefore, the aim of this review is to describe the typical clinical manifestations of vasculitides and their main radiologic features (especially AAV).
Keywords: antibodies; antineutrophil cytoplasmic; interstitial; lung diseases; multidetector computed tomography; vasculitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Jennette J.C., Falk R.J., Andrassy K., Bacon A.P., Churg J., Wolfgang L.G., Christiaan Hagen E., Hoffman G.S., Hunder G.G., Kallenberg C.G.M., et al. Nomenclature of systemic vasculitides: The proposal of an international consensus conference. Arthritis Rheum. 1994;37:187–192. doi: 10.1002/art.1780370206. - DOI - PubMed
-
- Maffessanti M., Dalpiaz G. Diffuse Lung Disease—Clinical Features, Pathology, HRCT. Springer; Berlin/Heidelberg, Germany: 2004.
Publication types
LinkOut - more resources
Full Text Sources
