

Translational Stroke Research Review: Using the Mouse to Model Human Futile Recanalization and Reperfusion Injury in Ischemic Brain Tissue
- PMID: 34943816
- PMCID: PMC8699609
- DOI: 10.3390/cells10123308
Translational Stroke Research Review: Using the Mouse to Model Human Futile Recanalization and Reperfusion Injury in Ischemic Brain Tissue
Abstract
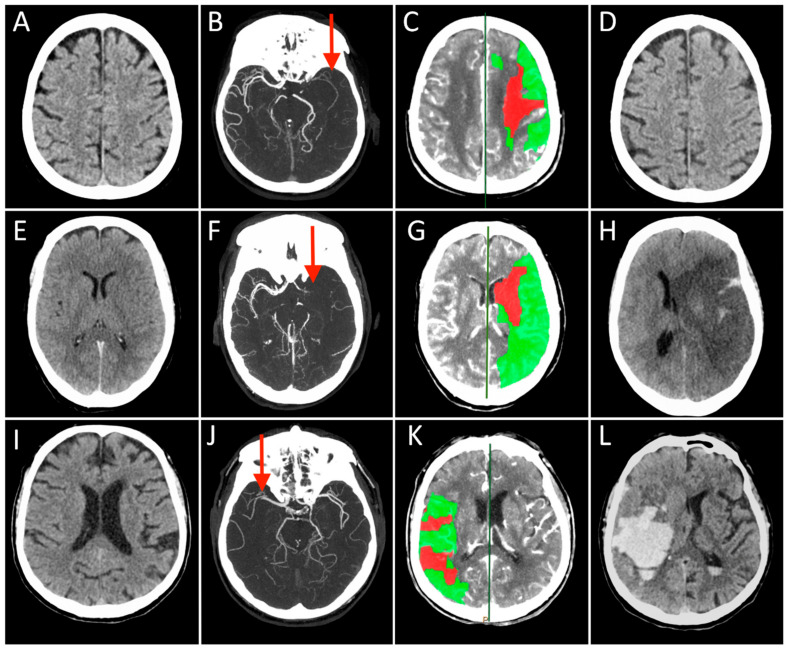
The approach to reperfusion therapies in stroke patients is rapidly evolving, but there is still no explanation why a substantial proportion of patients have a poor clinical prognosis despite successful flow restoration. This issue of futile recanalization is explained here by three clinical cases, which, despite complete recanalization, have very different outcomes. Preclinical research is particularly suited to characterize the highly dynamic changes in acute ischemic stroke and identify potential treatment targets useful for clinical translation. This review surveys the efforts taken so far to achieve mouse models capable of investigating the neurovascular underpinnings of futile recanalization. We highlight the translational potential of targeting tissue reperfusion in fully recanalized mouse models and of investigating the underlying pathophysiological mechanisms from subcellular to tissue scale. We suggest that stroke preclinical research should increasingly drive forward a continuous and circular dialogue with clinical research. When the preclinical and the clinical stroke research are consistent, translational success will follow.
Keywords: brain; futile recanalization; ischemic stroke; mechanical thrombectomy; reperfusion; translational stroke research.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Ter Schiphorst A., Charron S., Hassen W.B., Provost C., Naggara O., Benzakoun J., Seners P., Turc G., Baron J.C., Oppenheim C. Tissue no-reflow despite full recanalization following thrombectomy for anterior circulation stroke with proximal occlusion: A clinical study. J. Cereb. Blood Flow Metab. 2021;41:253–266. doi: 10.1177/0271678X20954929. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
