

Platelet Activation Mechanisms and Consequences of Immune Thrombocytopenia
- PMID: 34943895
- PMCID: PMC8699996
- DOI: 10.3390/cells10123386
Platelet Activation Mechanisms and Consequences of Immune Thrombocytopenia
Abstract
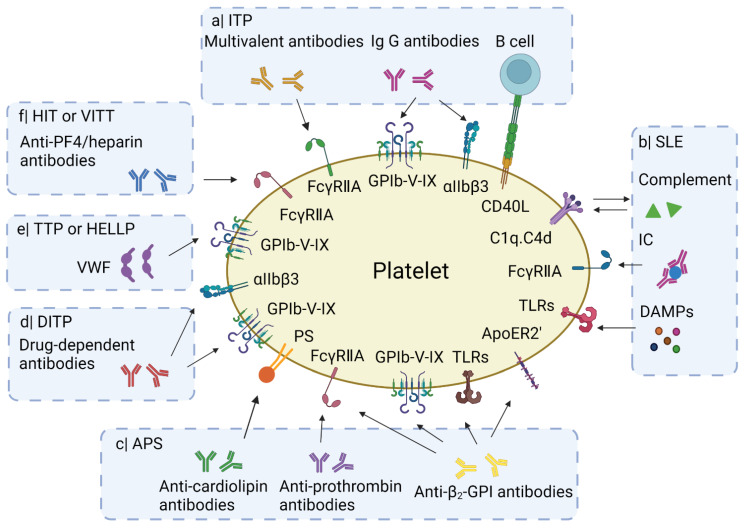
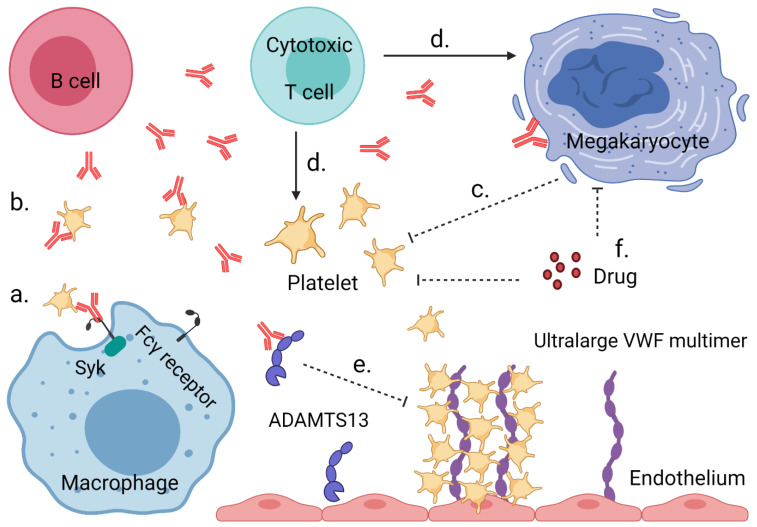
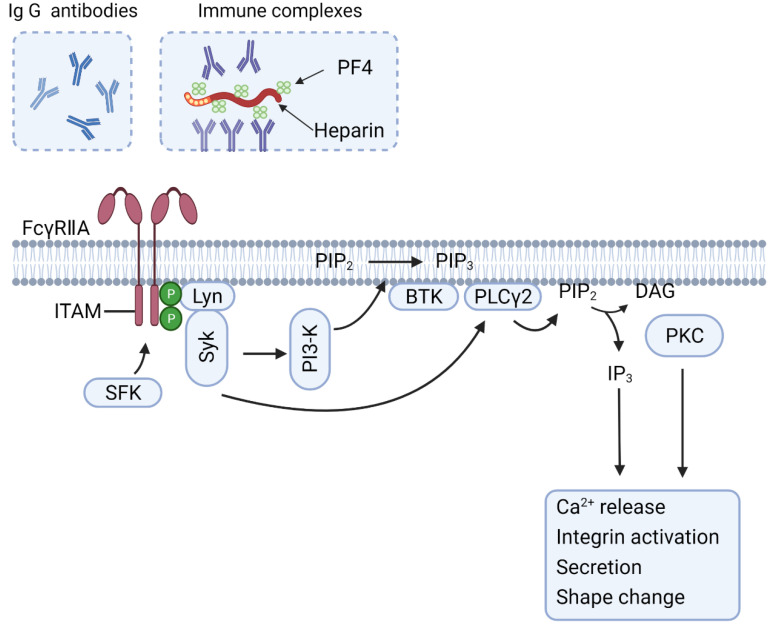
Autoimmune disorders are often associated with low platelet count or thrombocytopenia. In immune-induced thrombocytopenia (IIT), a common mechanism is increased platelet activity, which can have an increased risk of thrombosis. In addition, or alternatively, auto-antibodies suppress platelet formation or augment platelet clearance. Effects of the auto-antibodies are linked to the unique structural and functional characteristics of platelets. Conversely, prior platelet activation may contribute to the innate and adaptive immune responses. Extensive interplay between platelets, coagulation and complement activation processes may aggravate the pathology. Here, we present an overview of the reported molecular causes and consequences of IIT in the most common forms of autoimmune disorders. These include idiopathic thrombocytopenic purpura (ITP), systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), drug-induced thrombocytopenia (DITP), heparin-induced thrombocytopenia (HIT), COVID-19 vaccine-induced thrombosis with thrombocytopenia (VITT), thrombotic thrombocytopenia purpura (TTP), and hemolysis, the elevated liver enzymes and low platelet (HELLP) syndrome. We focus on the platelet receptors that bind auto-antibodies, the immune complexes, damage-associated molecular patterns (DAMPs) and complement factors. In addition, we review how circulating platelets serve as a reservoir of immunomodulatory molecules. By this update on the molecular mechanisms and the roles of platelets in the pathogenesis of autoimmune diseases, we highlight platelet-based pathways that can predispose for thrombocytopenia and are linked thrombotic or bleeding events.
Keywords: auto-antibodies; autoimmune disorders; immune thrombocytopenia; platelet; thrombosis.
Conflict of interest statement
S.S., B.d.L. and M.R. are employees of Synapse Research Institute Maastricht. P.G.d.G. and J.W.M.H. are consultants at Synapse Research Institute Maastricht. R.T.U. declares no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Grodzielski M., Goette N.P., Glembotsky A.C., Constanza Baroni Pietto M., Méndez-Huergo S.P., Pierdominici M.S., Montero V.S., Rabinovich G.A., Molinas F.C., Heller P.G., et al. Multiple concomitant mechanisms contribute to low platelet count in patients with immune thrombocytopenia. Sci. Rep. 2019;9:2208. doi: 10.1038/s41598-018-38086-1. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
