

Repetitive Trans Spinal Magnetic Stimulation Improves Functional Recovery and Tissue Repair in Contusive and Penetrating Spinal Cord Injury Models in Rats
- PMID: 34944643
- PMCID: PMC8698720
- DOI: 10.3390/biomedicines9121827
Repetitive Trans Spinal Magnetic Stimulation Improves Functional Recovery and Tissue Repair in Contusive and Penetrating Spinal Cord Injury Models in Rats
Abstract
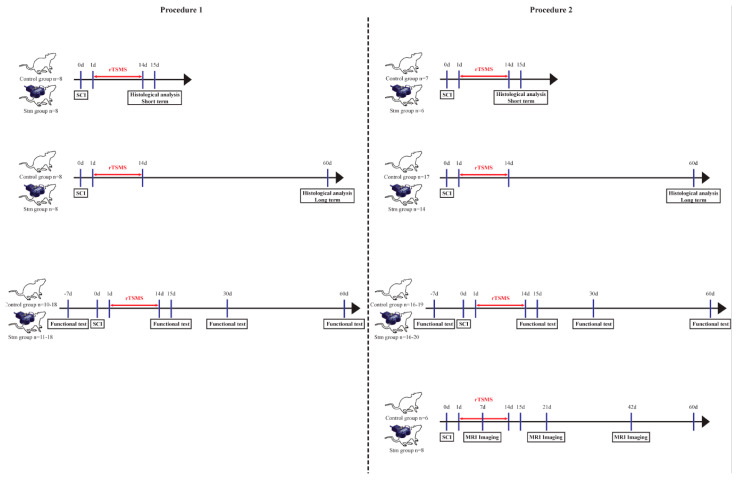
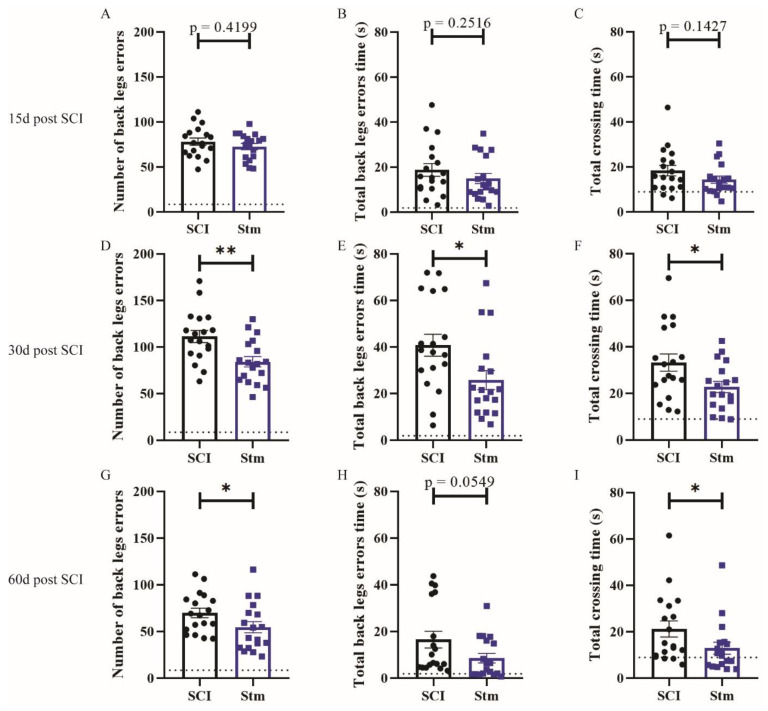
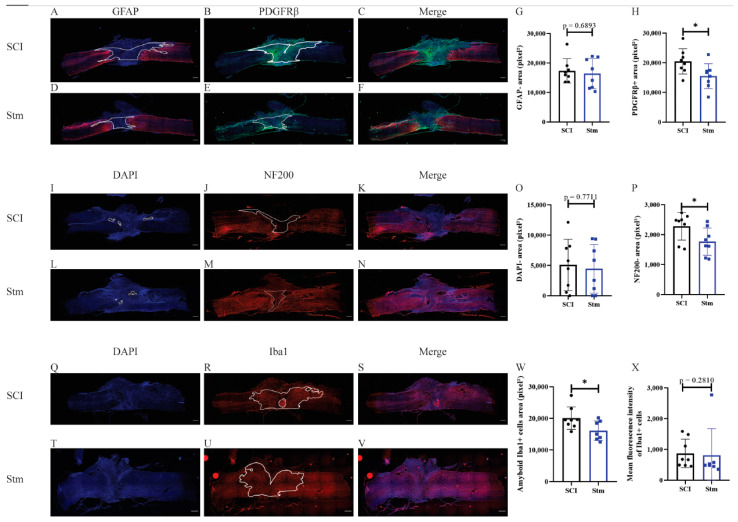
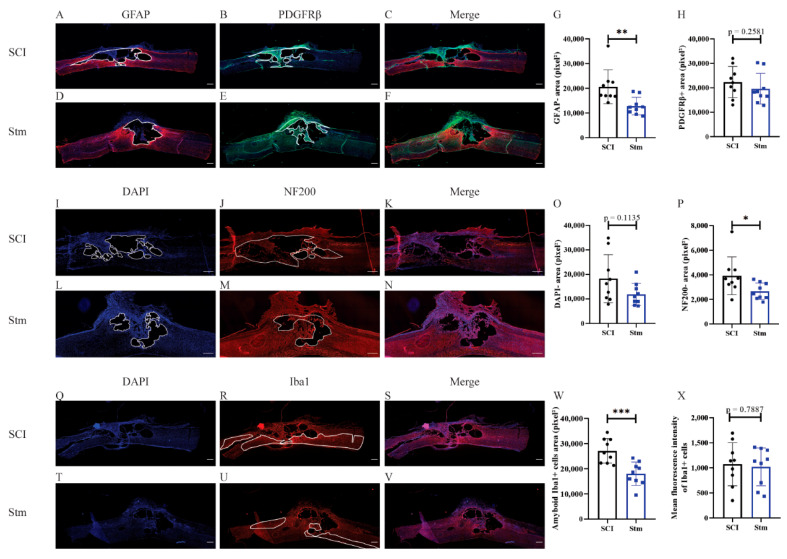
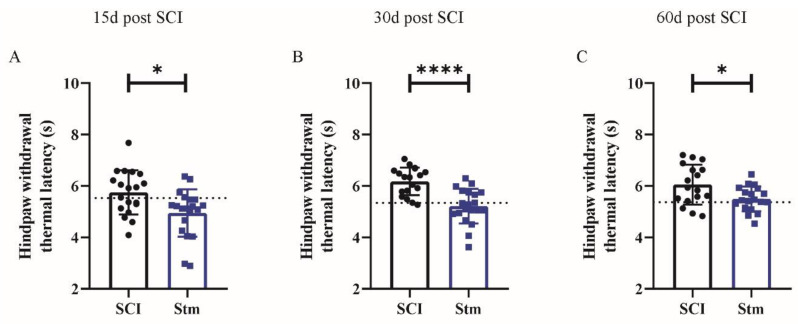
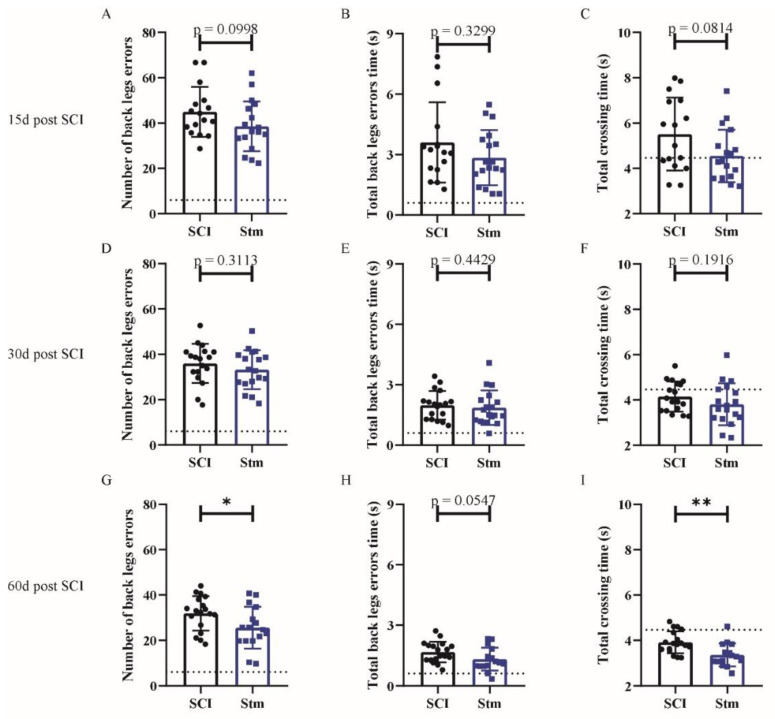
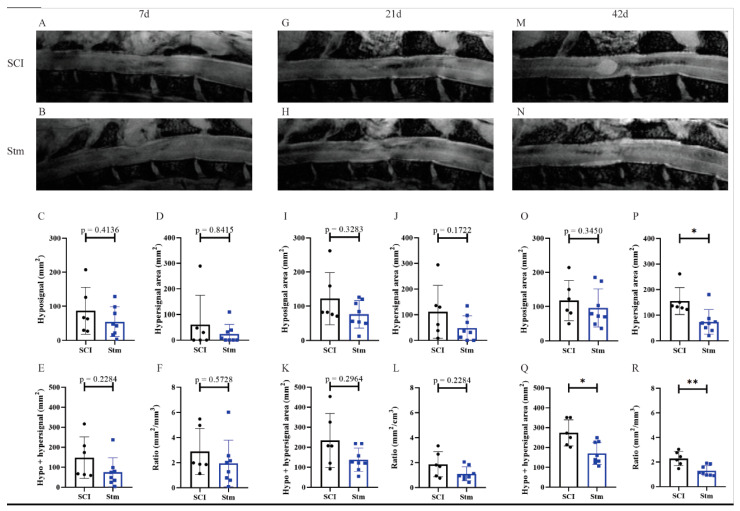
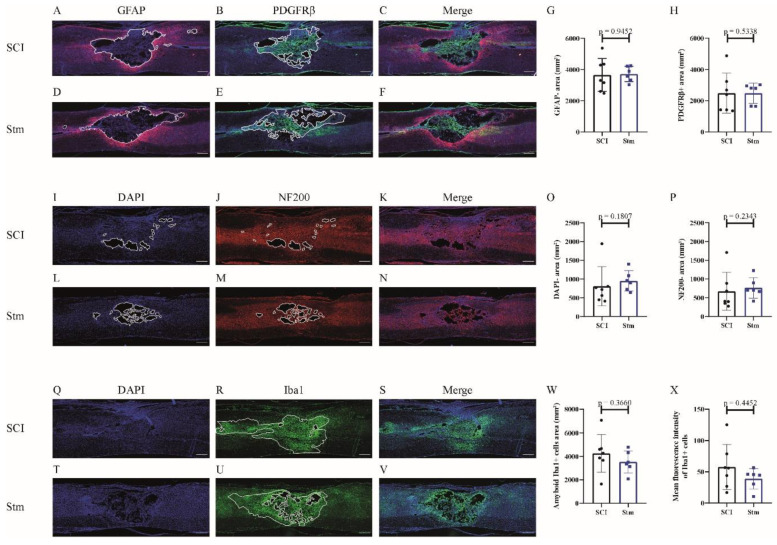
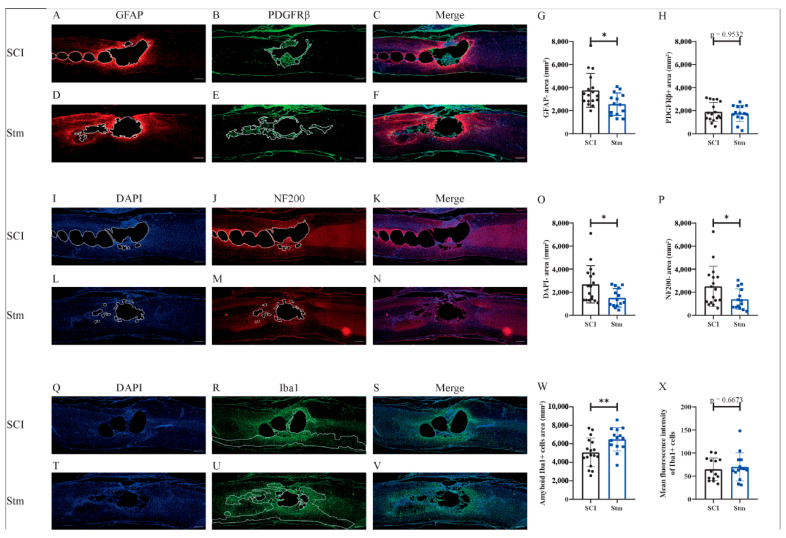
Spinal cord injury (SCI) is an incurable condition in which the brain is disconnected partially or completely from the periphery. Mainly, SCIs are traumatic and are due to traffic, domestic or sport accidents. To date, SCIs are incurable and, most of the time, leave the patients with a permanent loss of sensitive and motor functions. Therefore, for several decades, researchers have tried to develop treatments to cure SCI. Among them, recently, our lab has demonstrated that, in mice, repetitive trans-spinal magnetic stimulation (rTSMS) can, after SCI, modulate the lesion scar and can induce functional locomotor recovery non-invasively. These results are promising; however, before we can translate them to humans, it is important to reproduce them in a more clinically relevant model. Indeed, SCIs do not lead to the same cellular events in mice and humans. In particular, SCIs in humans induce the formation of cystic cavities. That is why we propose here to validate the effects of rTSMS in a rat animal model in which SCI leads to the formation of cystic cavities after penetrating and contusive SCI. To do so, several techniques, including immunohistochemical, behavioral and MRI, were performed. Our results demonstrate that rTSMS, in both SCI models, modulates the lesion scar by decreasing the formation of cystic cavities and by improving axonal survival. Moreover, rTSMS, in both models, enhances functional locomotor recovery. Altogether, our study describes that rTSMS exerts positive effects after SCI in rats. This study is a further step towards the use of this treatment in humans.
Keywords: cystic cavities and functional recovery; glial scar; magnetic stimulation; rehabilitation; spinal cord injury.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
