

Conventional Transarterial Chemoembolization Versus Drug-Eluting Beads in Patients with Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
- PMID: 34944792
- PMCID: PMC8699068
- DOI: 10.3390/cancers13246172
Conventional Transarterial Chemoembolization Versus Drug-Eluting Beads in Patients with Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
Abstract
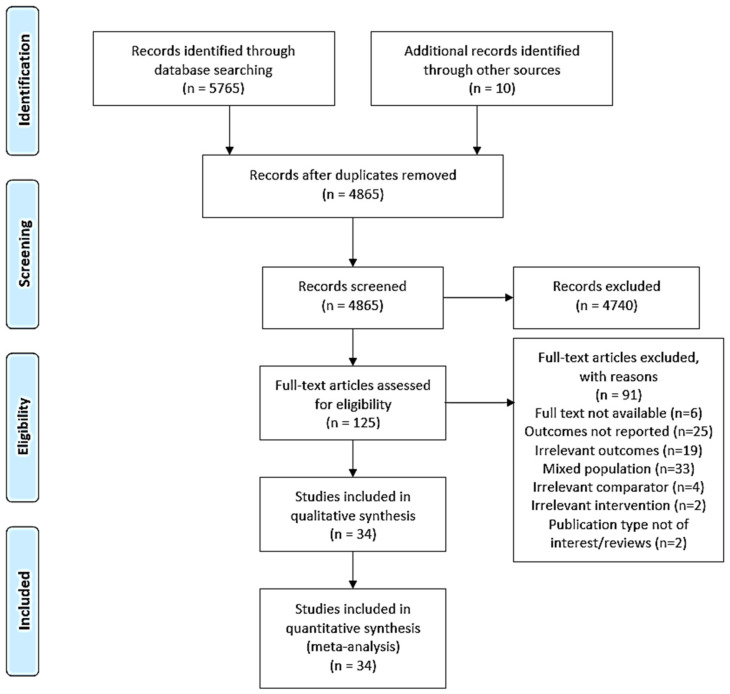
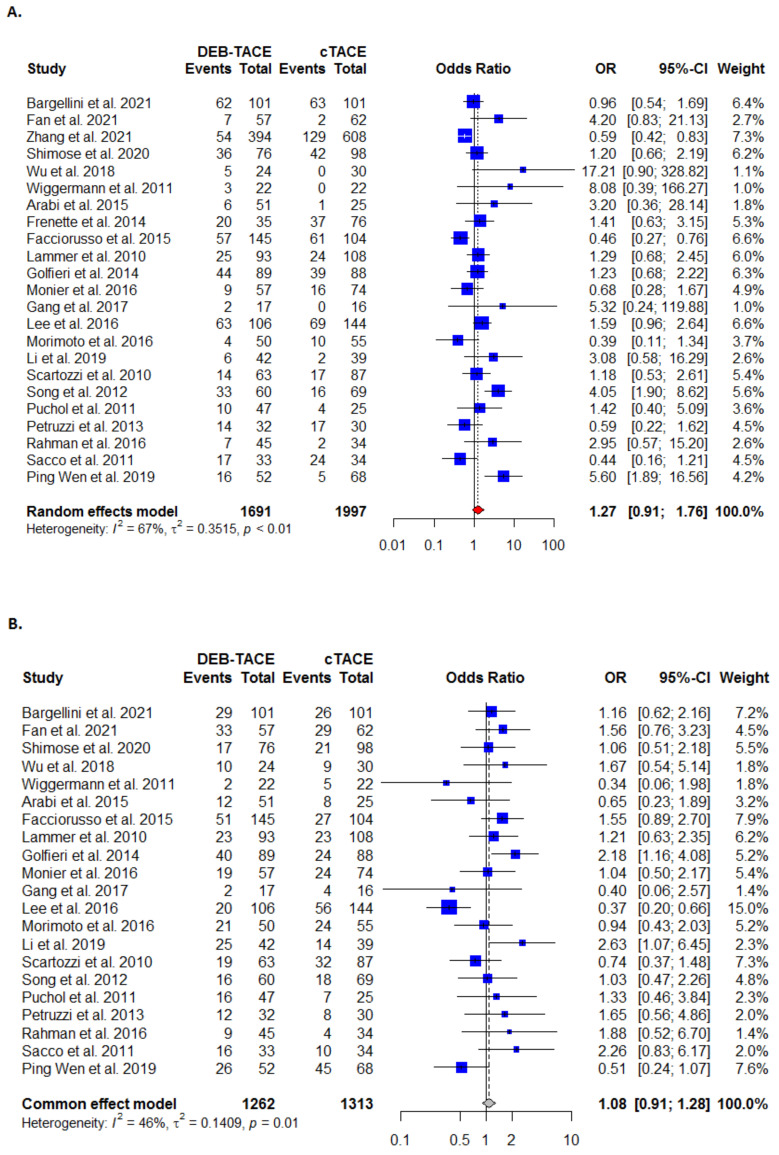
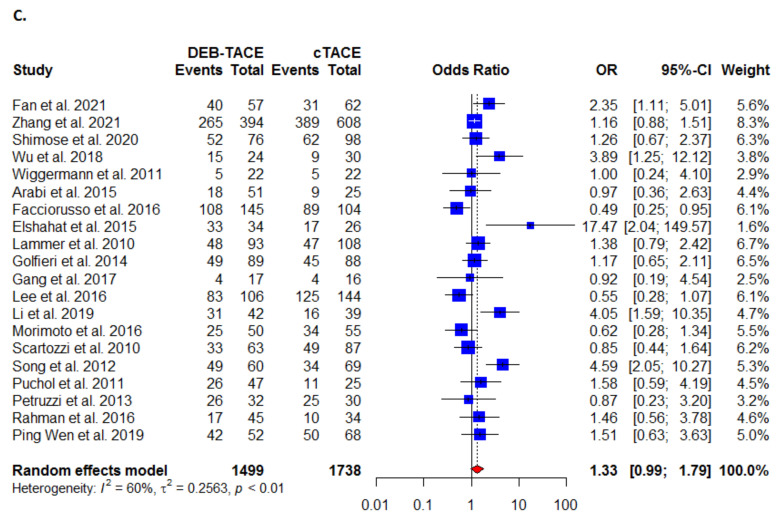
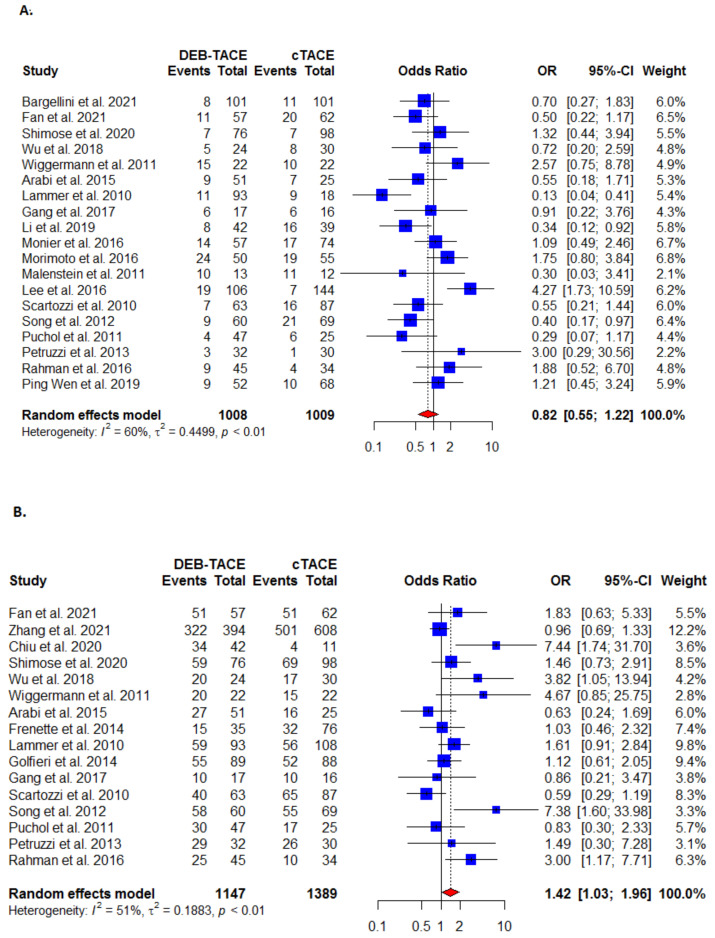
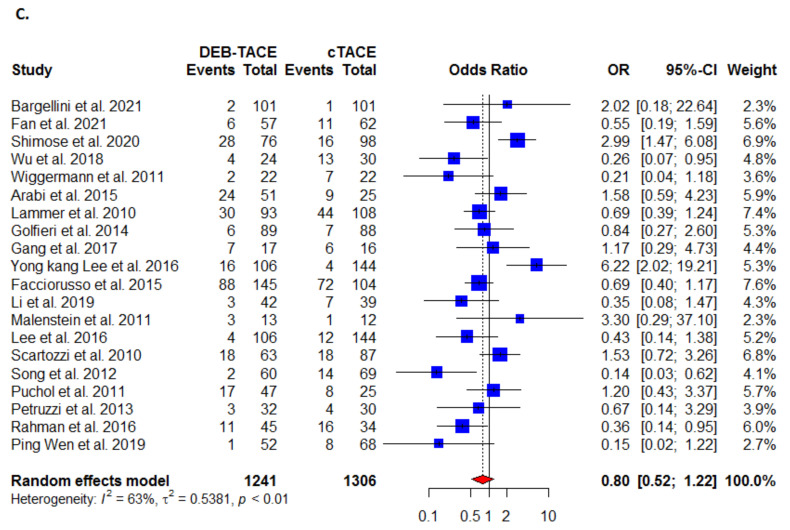
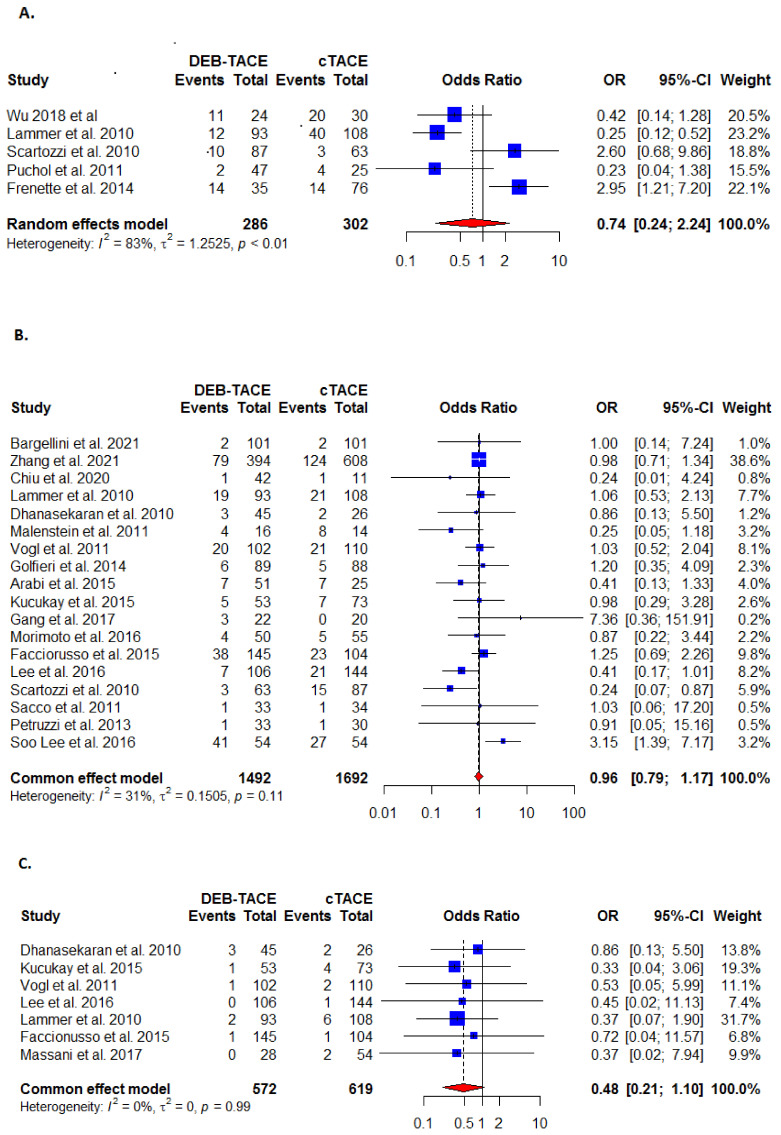
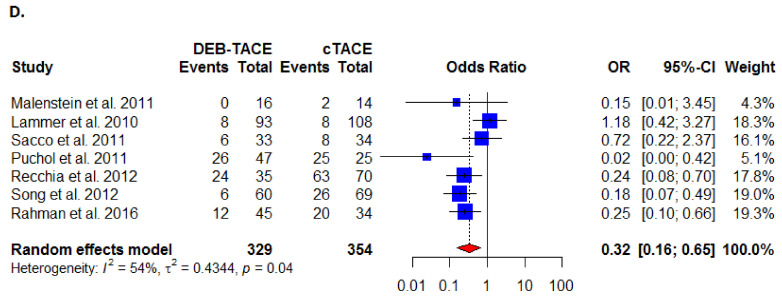
Hepatocellular carcinoma (HCC) occurs in nearly three-quarters of all primary liver cancers, with the majority not amenable to curative therapies. We therefore aimed to re-evaluate the safety, efficacy, and survival benefits of treating patients with drug-eluting beads transcatheter arterial chemoembolization (DEB-TACE) compared to the conventional transcatheter arterial chemoembolization (C-TACE). Several databases were searched with a strict eligibility criterion for studies reporting on adult patients with unresectable or recurrent HCC. The pooled analysis included 34 studies involving 4841 HCC patients with a median follow-up of 1.5 to 18 months. There were no significant differences between DEB-TACE and C-TACE with regard to complete response, partial response and disease stability. However, disease control (OR: 1.42 (95% CI (1.03,1.96) and objective response (OR: 1.33 (95% CI (0.99, 1.79) were significantly more effective for DEB-TACE treatment with fewer severe complications and all-cause mortality. The pooled-analysis did not find superiority of DEB-TACE in complete or partial response, disease stability, controlling disease progression, and 30 day or end-mortality. However, results showed that DEB-TACE is associated with a better objective response, disease control, and lower all-cause mortality with severe complications compared to C-TACE treatment. Given that the safety outcomes are based on limited studies with a potential for bias, there was no clear improvement of DEB-TACE over C-TACE treatment.
Keywords: drug-eluting beads; hepatocellular carcinoma; transarterial chemoembolization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Fitzmaurice C., Allen C., Barber R.M., Barregard L., Bhutta Z.A., Brenner H., Dicker D.J., Chimed-Orchir O., Dandona R., Dandona L., et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017;3:524–548. - PMC - PubMed
-
- Mohammadian M., Mahdavifar N., Mohammadian-Hafshejani A., Salehiniya H. Liver cancer in the world: Epidemiology, incidence, mortality and risk factors. World Cancer Res. J. 2018;5:e1082.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
