

Adjuvant Hysterectomy for Cervical Cancer Patients Treated with Chemoradiation Therapy: A Systematic Review on the Pathology-Proven Residual Disease Rate
- PMID: 34944810
- PMCID: PMC8699574
- DOI: 10.3390/cancers13246190
Adjuvant Hysterectomy for Cervical Cancer Patients Treated with Chemoradiation Therapy: A Systematic Review on the Pathology-Proven Residual Disease Rate
Abstract
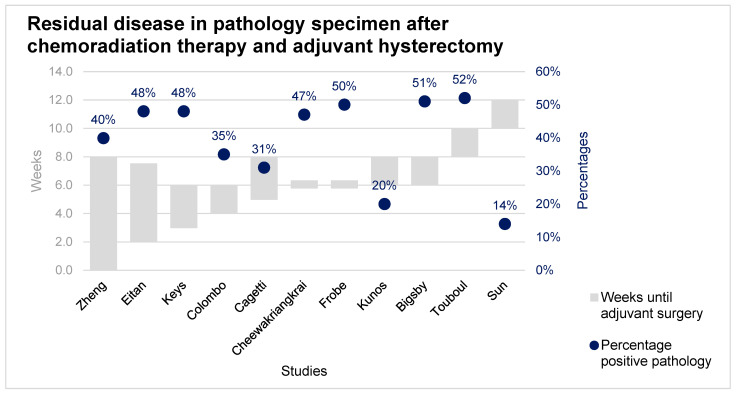
Objective: To determine the incidence of pathology-proven residual disease in adjuvant hysterectomy specimens in patients with cervical cancer, treated with chemoradiation therapy. Secondly, to assess a possible association for pathology-proven residual disease regarding the time between chemoradiation therapy and adjuvant hysterectomy. Additionally, the survival rate and complication rate were assessed.
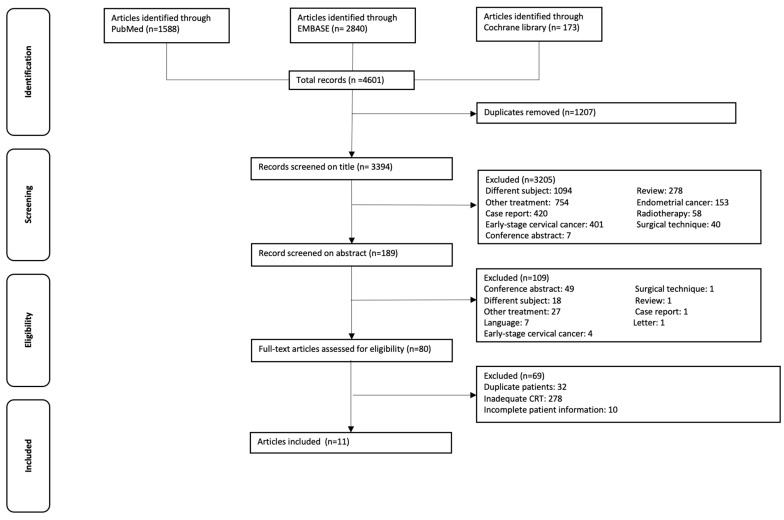
Methods: PubMed, EMBASE, and the Cochrane database were searched from inception up to 8 March 2021.
Results: Of the 4601 screened articles, eleven studies were included. A total of 1205 patients were treated with chemoradiation therapy and adjuvant hysterectomy, ranging from three to twelve weeks after chemoradiation therapy. A total of 411 out of 1205 patients (34%) had pathology-proven residual disease in the adjuvant hysterectomy specimen. There was no association found in the time between chemoradiation therapy and adjuvant hysterectomy. Follow-up ranged from 2.4 to 245 months, during which 270 patients (22%) relapsed, and 298 patients (27%) were deceased. A total of 202 (35%) complications were registered in 578 patients.
Conclusion: there is no association found in the time between chemoradiation therapy and residual disease on adjuvant hysterectomy specimens. The survival rates after chemoradiation therapy and adjuvant hysterectomy are suboptimal, while the risk of complications after adjuvant hysterectomy is high.
Keywords: adjuvant hysterectomy; chemoradiation therapy; complications; locally advanced cervical cancer; survival.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO Cervical Cancer 2019. [(accessed on 2 December 2020)]. Available online: https://www.who.int/cancer/prevention/diagnosis-screening/cervical-cance...
-
- Cancer Research UK Cancer Statistics for the UK. [(accessed on 14 January 2020)]. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics-f....
-
- Cibula D., Pötter R., Planchamp F., Avall-Lundqvist E., Fischerova D., Haie Meder C., Köhler C., Landoni F., Lax S., Lindegaard J.C., et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients With Cervical Cancer. Int. J. Gynecol. Cancer. 2018;472:641–655. doi: 10.1097/IGC.0000000000001216. - DOI - PubMed
-
- Eifel P.J., Winter K., Morris M., Levenback C., Grigsby P.W., Cooper J., Rotman M., Gershenson D., Mutch D.G. Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: An update of Radiation Therapy Oncology Group Trial (RTOG) 90-01. J. Clin. Oncol. 2004;22:872–880. doi: 10.1200/JCO.2004.07.197. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
