

Contact X-ray Brachytherapy for Older or Inoperable Rectal Cancer Patients: Short-Term Oncological and Functional Follow-Up
- PMID: 34944953
- PMCID: PMC8699080
- DOI: 10.3390/cancers13246333
Contact X-ray Brachytherapy for Older or Inoperable Rectal Cancer Patients: Short-Term Oncological and Functional Follow-Up
Abstract
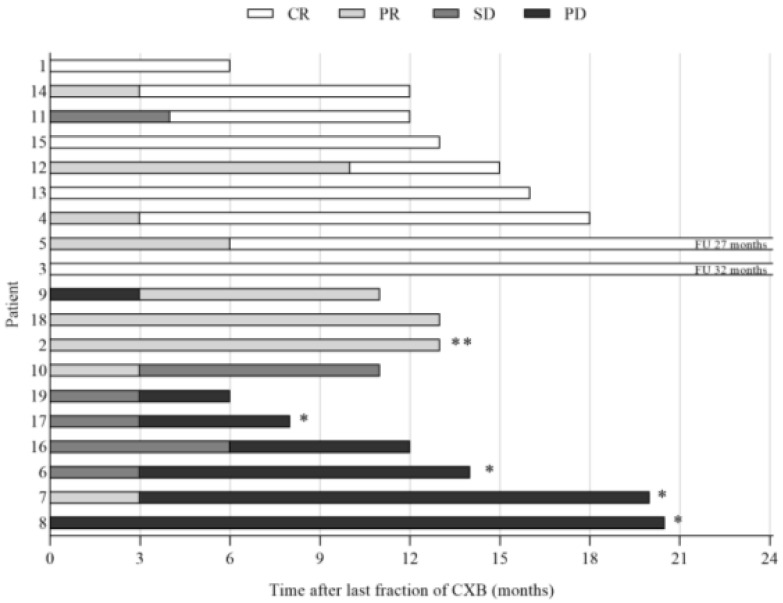
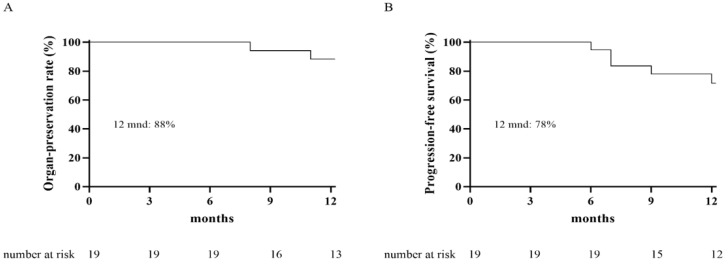
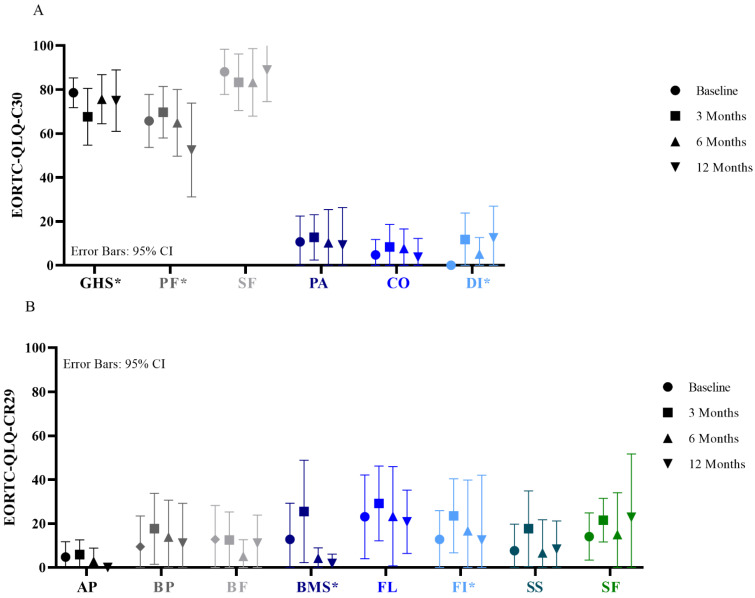
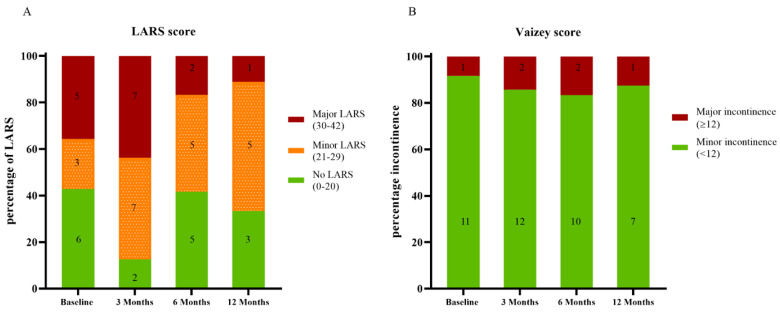
Total mesorectal excision for rectal cancer is a major operation associated with morbidity and mortality. For older or inoperable patients, alternatives are necessary. This prospective study evaluated the oncological and functional outcome and quality of life of older or inoperable rectal cancer patients treated with a contact X-ray brachytherapy boost to avoid major surgery. During follow-up, tumor response and toxicity on endoscopy were scored. Functional outcome and quality of life were assessed with self-administered questionnaires. Additionally, in-depth interviews regarding patients' experiences were conducted. Nineteen patients were included with a median age of 80 years (range 72-91); nine patients achieved a clinical complete response and in another four local control of the tumor was established. The 12 month organ-preservation rate, progression-free survival, and overall survival were 88%, 78%, and 100%, respectively. A transient decrease in quality of life and bowel function was observed at 3 months, which was generally restored at 6 months. In-depth interviews revealed that patients' experience was positive despite the side-effects shortly after treatment. In older or inoperable rectal cancer patients, contact X-ray brachytherapy can be considered an option to avoid total mesorectal excision. Contact X-ray brachytherapy is well-tolerated and can provide good tumor control.
Keywords: contact X-ray brachytherapy; functional outcome; older patients; oncological outcome; quality of life; rectal cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Chen T.Y.-T., Wiltink L.M., Nout R.A., Meershoek-Klein Kranenbarg E., Laurberg S., Marijnen C.A., van de Velde C.J. Bowel function 14 years after preoperative short-course radiotherapy and total mesorectal excision for rectal cancer: Report of a multicenter randomized trial. Clin. Colorectal Cancer. 2015;14:106–114. doi: 10.1016/j.clcc.2014.12.007. - DOI - PubMed
LinkOut - more resources
Full Text Sources
