

The Impact of the FilmArray-Based Detection of Microbial Pathogens from Positive Blood Culture Vials on the Time to Optimal Antimicrobial Regimen in Intensive Care Units of the Helios University Clinic Wuppertal, Germany
- PMID: 34945183
- PMCID: PMC8704407
- DOI: 10.3390/jcm10245880
The Impact of the FilmArray-Based Detection of Microbial Pathogens from Positive Blood Culture Vials on the Time to Optimal Antimicrobial Regimen in Intensive Care Units of the Helios University Clinic Wuppertal, Germany
Abstract
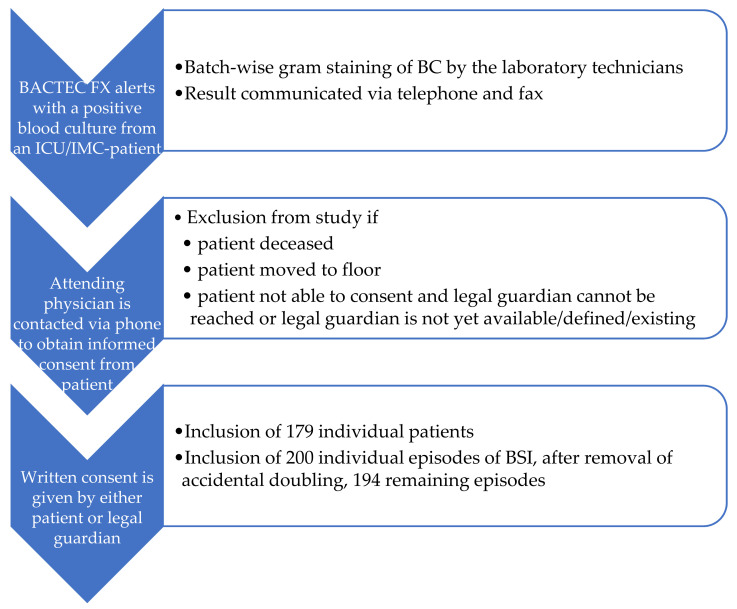
The role of empirical therapy and time to first effective treatment, including the antimicrobial stewardship program, are decisive in patients presenting with bloodstream infections (BSI). The FilmArray® Blood Culture Identification Panel (FA BCID 1.0) detects 24 bacterial and fungal pathogens as well as 3 resistance genes from positive blood cultures in approximately 70 min. In this paper, we evaluate the impact of the additional FA BCID analysis on the time to an optimal antimicrobial therapy and on the length of stay in the ICU, ICU mortality, and PCT level reduction. This retro-/prospective trial was conducted in BSI patients in the ICU at a German tertiary care hospital. A total of 179 individual patients with 200 episodes of BSI were included in the prospective intervention group, and 150 patients with 170 episodes of BSI in the retrospective control group. In the intervention group, BSI data were analyzed including the MALDI-TOF MS (matrix assisted laser desorption ionization time-of-flight mass spectrometry) and FA BCID results from January 2019 to August 2020; the data from the control group, including the MALDI-TOF results, were collected retrospectively from the year 2018. The effective and appropriate antimicrobial regimen occurred in a median of 17 hours earlier in the intervention versus control group (p = 0.071). Furthermore, changes in the antimicrobial regimens of the intervention group that did not immediately lead to an optimal therapy occurred significantly earlier by a median of 24 hours (p = 0.029). Surrogate markers, indicating an earlier recovery of the patients from the intervention group, such as length of stay at the ICU, duration of mechanical ventilation, or an earlier reduction in PCT level, were not significantly affected. However, mortality did not differ between the patient groups. A postulated reduction of the antimicrobial therapy, in those cases in which coagulase-negative Staphylococcus species were identified, did occur in the control group, but not in the intervention group (p = 0.041). The implementation of FA BCID into the laboratory workflow can improve patient care by optimizing antimicrobial regimen earlier in BSI patients as it provides rapid and accurate results for key pathogens associated with BSI, as well as important antimicrobial resistance markers, e.g., mecA or vanA.
Keywords: ICU; RT PCR; antibiotic resistance; appropriate antimicrobial regimen; blood culture; bloodstream infections; identification of pathogens; length of stay; sepsis; septic shock; ventilation duration.
Conflict of interest statement
The authors report no conflict of interest. There are no other financial or non-financial competing interest for this manuscript.
Figures
References
-
- Rhodes A., Evans L.E., Alhazzani W., Levy M.M., Antonelli M., Ferrer R., Kumar A., Sevransky J.E., Sprung C.L., Nunnally M.E., et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017;43:304–377. doi: 10.1007/s00134-017-4683-6. - DOI - PubMed
-
- Ferrer R., Martin-Loeches I., Phillips G., Osborn T.M., Townsend S., Dellinger R.P., Artigas A., Schorr C., Levy M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014;42:1749–1755. doi: 10.1097/CCM.0000000000000330. - DOI - PubMed
-
- Kumar A., Roberts D., Wood K.E., Light B., Parrillo J.E., Sharma S., Suppes R., Feinstein D., Zanotti S., Taiberg L., et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006;34:1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
