

A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome
- PMID: 34945213
- PMCID: PMC8708187
- DOI: 10.3390/jcm10245913
A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome
Abstract
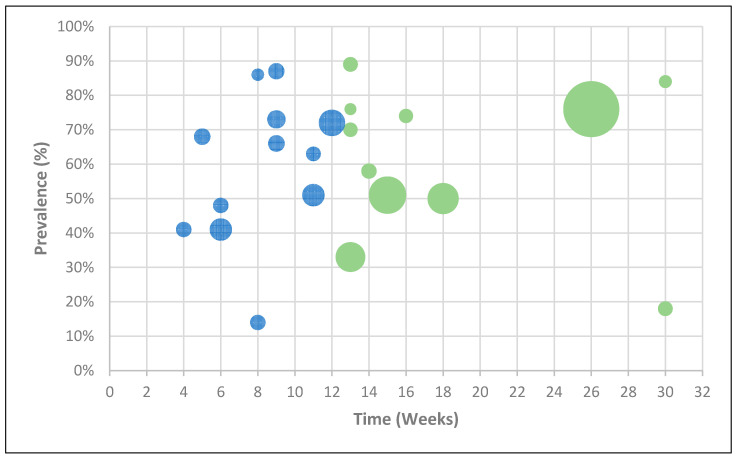
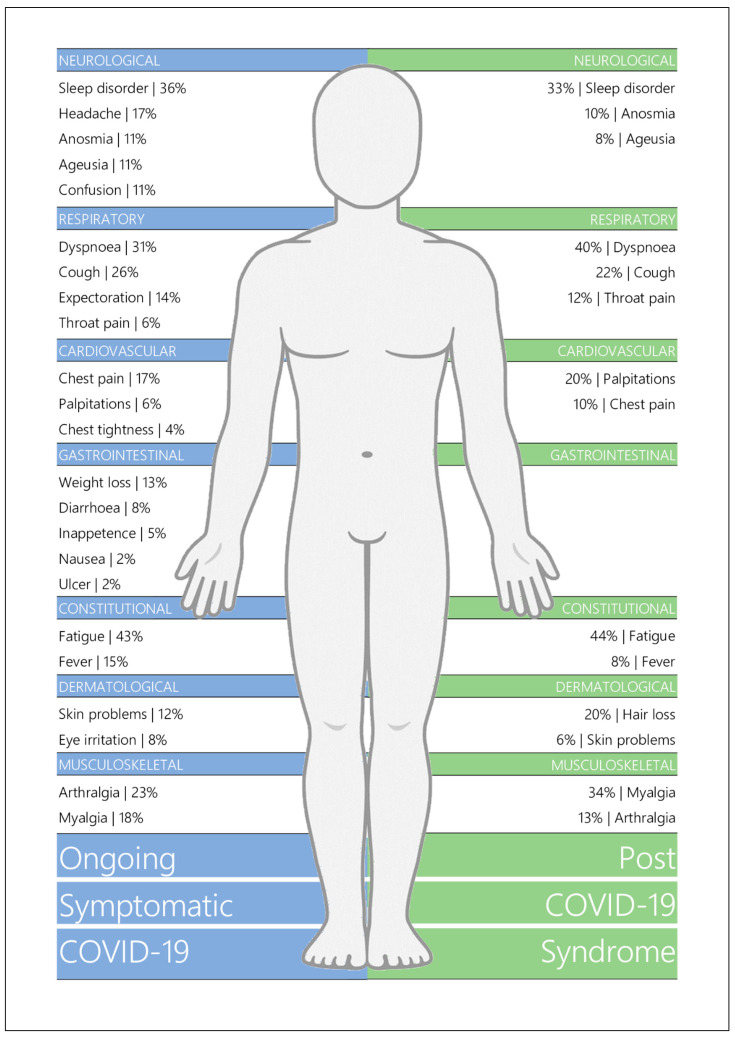
Objective: To compare the two phases of long COVID, namely ongoing symptomatic COVID-19 (OSC; signs and symptoms from 4 to 12 weeks from initial infection) and post-COVID-19 syndrome (PCS; signs and symptoms beyond 12 weeks) with respect to symptomatology, abnormal functioning, psychological burden, and quality of life.
Design: Systematic review.
Data sources: Electronic search of EMBASE, MEDLINE, ProQuest Coronavirus Research Database, LitCOVID, and Google Scholar between January and April 2021, and manual search for relevant citations from review articles. Eligibility Criteria: Cross-sectional studies, cohort studies, randomised control trials, and case-control studies with participant data concerning long COVID symptomatology or abnormal functioning.
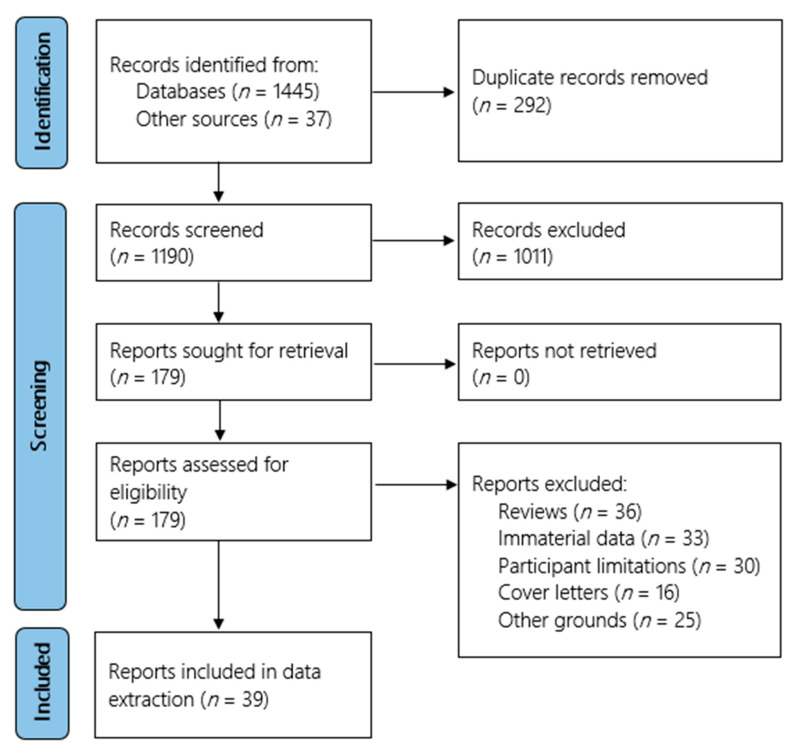
Data extraction: Studies were screened and assessed for risk of bias by two independent reviewers, with conflicts resolved with a third reviewer. The AXIS tool was utilised to appraise the quality of the evidence. Data were extracted and collated using a data extraction tool in Microsoft Excel.
Results: Of the 1145 studies screened, 39 were included, all describing adult cohorts with long COVID and sample sizes ranging from 32 to 1733. Studies included data pertaining to symptomatology, pulmonary functioning, chest imaging, cognitive functioning, psychological disorder, and/or quality of life. Fatigue presented as the most prevalent symptom during both OSC and PCS at 43% and 44%, respectively. Sleep disorder (36%; 33%), dyspnoea (31%; 40%), and cough (26%; 22%) followed in prevalence. Abnormal spirometry (FEV1 < 80% predicted) was observed in 15% and 11%, and abnormal chest imaging was observed in 34% and 28%, respectively. Cognitive impairments were also evident (20%; 15%), as well as anxiety (28%; 34%) and depression (25%; 32%). Decreased quality of life was reported by 40% in those with OSC and 57% with PCS.
Conclusions: The prevalence of OSC and PCS were highly variable. Reported symptoms covered a wide range of body systems, with a general overlap in frequencies between the two phases. However, abnormalities in lung function and imaging seemed to be more common in OSC, whilst anxiety, depression, and poor quality of life seemed more frequent in PCS. In general, the quality of the evidence was moderate and further research is needed to understand longitudinal symptomatology trajectories in long COVID. Systematic Review Registration: Registered with PROSPERO with ID #CRD42021247846.
Keywords: COVID-19; fatigue; long COVID; ongoing symptomatic COVID-19; post-COVID-19 syndrome; symptomatology.
Conflict of interest statement
The authors declare there is no conflicts of interest.
Figures
References
-
- World Health Organisation WHO Coronavirus (COVID-19) Dashboard: World Health Organisation. 2021. [(accessed on 5 December 2021)]. Available online: https://covid19.who.int/
-
- Grant M.C., Geoghegan L., Arbyn M., Mohammed Z., McGuinness L., Clarke E.L., Wade R.G. The Prevalence of Symptoms in 24,410 Adults Infected by the Novel Coronavirus (SARS-CoV-2; COVID-19): A Systematic Review and Meta-Analysis of 148 Studies from 9 Countries. PLoS ONE. 2020;15:e0234765. doi: 10.1371/journal.pone.0234765. - DOI - PMC - PubMed
-
- Pijls B.G., Jolani S., Atherley A., Derckx R.T., Dijkstra J.I.R., Franssen G.H.L., Hendriks S., Richters A., Venemans-Jellema A., Zalpuri S., et al. Demographic Risk Factors for COVID-19 Infection, Severity, ICU Admission and Death: A Meta-Analysis of 59 Studies. BMJ Open. 2021;11:e044640. doi: 10.1136/bmjopen-2020-044640. - DOI - PMC - PubMed
-
- National Institute for Health and Care Excellence . COVID-19 Rapid Guideline: Managing COVID-19. NICE; London, UK: 2021. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
