

Different Effects of Empagliflozin on Markers of Mineral-Bone Metabolism in Diabetic and Non-Diabetic Patients with Stage 3 Chronic Kidney Disease
- PMID: 34946298
- PMCID: PMC8705759
- DOI: 10.3390/medicina57121352
Different Effects of Empagliflozin on Markers of Mineral-Bone Metabolism in Diabetic and Non-Diabetic Patients with Stage 3 Chronic Kidney Disease
Abstract
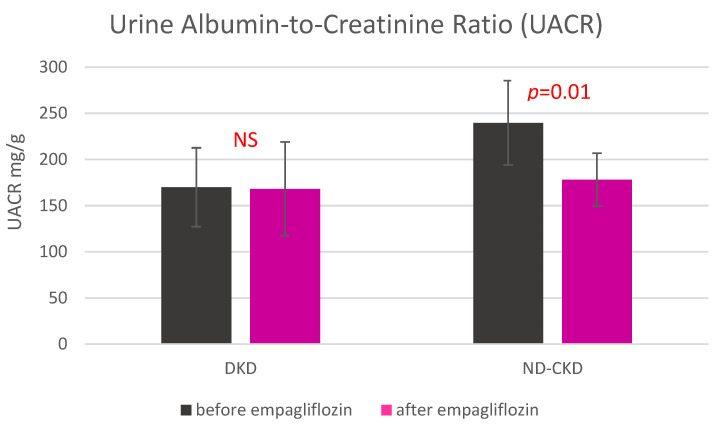
Background and objectives: Treatment with sodium-glucose co-transporter 2 (SGLT2) inhibitors decrease tubular reabsorption of phosphate, which may explain the reduction of bone mineral density and an excess of bone fractures observed in some studies with this class of drugs. Since an increased risk of bone fractures may also be a result of diabetes itself, our study aimed to compare the effect of empagliflozin on the markers of mineral-bone metabolism between diabetic (DKD) and non-diabetic (ND-CKD) patients with stage 3 chronic kidney disease (CKD). Materials and Methods: Forty-two patients with stage 3 CKD and A2 albuminuria, including 18 with DKD and 24 ND-CKD, were investigated. All subjects received 10 mg empagliflozin for 7 days. Serum calcium, phosphate, parathormone (PTH), calcitriol, bone alkaline phosphatase (BAP), FGF-23 and urine calcium, phosphate, albumin and the renal tubular maximum reabsorption rate of phosphate to the glomerular filtration rate (TmP-GFR) were measured before and after empagliflozin administration. Differences in biomarkers response to empagliflozin between DKD and ND-CKD were the main measures of outcome. Results: There was a significant increase of PTH, FGF-23 and phosphate in DKD but not in ND-CKD whereas BAP and TmP/GFR did not change in either group. The reduction of albuminuria was only significant in ND-CKD. Conclusions: The effect of SGLT2 inhibitor on serum mineral and bone markers and on albuminuria in patients with CKD may be differently modified by the presence of diabetes mellitus.
Keywords: SGLT-2 inhibitors; albuminuria; calcium; diabetic kidney disease; phosphate; phosphatonins.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Figures
References
-
- Tentori F., Blayney M.J., Albert J.M., Gillespie B.W., Kerr P.G., Bommer J., Young E.W., Akizawa T., Akiba T., Pisoni R.L., et al. Mortality risk for dialysis patients with different levels of serum calcium, phosphate, and PTH: The Dialysis Outcomes and Practice Patterns Study (DOPPS) Am. J. Kidney Dis. 2008;52:519–530. doi: 10.1053/j.ajkd.2008.03.020. - DOI - PubMed
-
- Kandula P., Dobre M., Schold J.D., Schreiber M.J., Mehrotra R., Navaneethan S.D. Vitamin D supplementation in chronic kidney disease: A systematic review and meta-analysis of observational studies and randomized controlled trials. Clin. J. Am. Soc. Nephrol. 2011;6:50–62. doi: 10.2215/CJN.03940510. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
