

Pharmacists as accessible health care providers: quantifying the opportunity
- PMID: 34949110
- PMCID: PMC8890748
- DOI: 10.18553/jmcp.2022.28.1.85
Pharmacists as accessible health care providers: quantifying the opportunity
Abstract
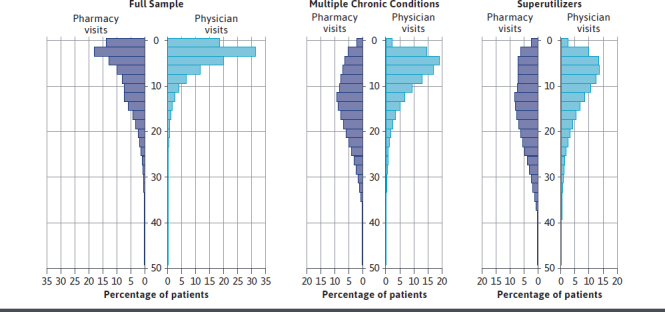
BACKGROUND: Community pharmacists are well positioned to improve patient access to care, which may assist value-based care programs in reaching patients. While pharmacy accessibility is broadly acknowledged, much of the research supporting accessibility claims is poor quality. OBJECTIVE: To quantify the accessibility of pharmacists in comparison with physicians or qualified health care professionals (QHP) in a commercially insured population. METHODS: IBM MarketScan claims data from 2018 were used for this cross-sectional study. Beneficiaries included in the primary analysis were aged 18-64 years, enrolled with pharmacy benefits in 2018 for 12 months, and had at least 1 valid prescription drug claim or evaluation and management (E&M) code in 2018. Unique pharmacy visits were defined using a 6-day fill window for prescription fill dates, while visits to physicians or other QHP were defined as unique service dates tied to an E&M code. We assessed differences in visit frequency for the full sample, those with multiple chronic conditions (MCC), and "superutilizers" (top 5% based on total cost of care). Our statistical approach included descriptive statistics and the Wilcoxon sign rank test. RESULTS: After applying the inclusion criteria, 11,720,958 beneficiaries were included in the full sample. The MCC cohort contained 13.8% of the total sample (mean [SD] age: 50.8 [10.8]; 908,880 [56.1%] female). Finally, the superutilizers were 57.3% female with an average age of 48.4 years and comprised 5.3% of the total sample. The median number of pharmacy and physician or QHP visits for the full sample were 5 and 3 (P < 0.0001), yielding a pharmacy to physician or QHP visit ratio of 1.7:1. The MCC cohort had a median of 13 pharmacy visits and 7 physician or QHP visits (ratio 1.9:1; P < 0.0001), and the superutilizers had a median of 14 pharmacy visits and 9 physician or QHP visits (ratio 1.6:1; P < 0.0001). CONCLUSIONS: This study found that patients visit their community pharmacies almost twice as often as they visit their physicians or other QHP. Study findings emphasize the accessibility of community pharmacists and highlight the role of community pharmacists in improving patient engagement in all care programs, including value-based care programs. DISCLOSURES: The database infrastructure used for this project was funded by the Department of Epidemiology, University of North Carolina (UNC) Gillings School of Global Public Health; the Cecil G. Sheps Center for Health Services Research, UNC; the CER Strategic Initiative of UNC's Clinical Translational Science Award (UL1TR001111); and the UNC School of Medicine. All authors are employed by the UNC School of Pharmacy. Urick declares consulting fees from Cardinal Health. The other authors have no conflicts of interest to disclose. Portions of this work were previously presented at the AMCP 2021 Virtual, April 12-16, 2021.
Conflict of interest statement
The database infrastructure used for this project was funded by the Department of Epidemiology, University of North Carolina (UNC) Gillings School of Global Public Health; the Cecil G. Sheps Center for Health Services Research, UNC; the CER Strategic Initiative of UNC’s Clinical Translational Science Award (UL1TR001111); and the UNC School of Medicine. All authors are employed by the UNC School of Pharmacy. Urick declares consulting fees from Cardinal Health. The other authors have no conflicts of interest to disclose.
Portions of this work were previously presented at the AMCP 2021 Virtual, April 12-16, 2021.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
