

Growth in achondroplasia including stature, weight, weight-for-height and head circumference from CLARITY: achondroplasia natural history study-a multi-center retrospective cohort study of achondroplasia in the US
- PMID: 34949201
- PMCID: PMC8697459
- DOI: 10.1186/s13023-021-02141-4
Growth in achondroplasia including stature, weight, weight-for-height and head circumference from CLARITY: achondroplasia natural history study-a multi-center retrospective cohort study of achondroplasia in the US
Abstract
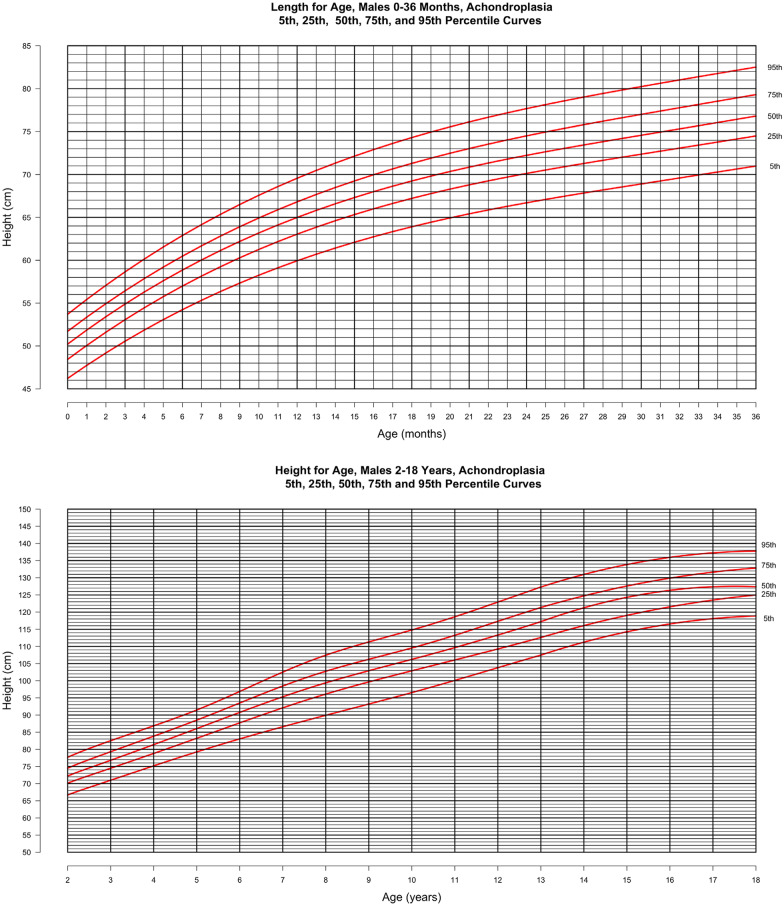
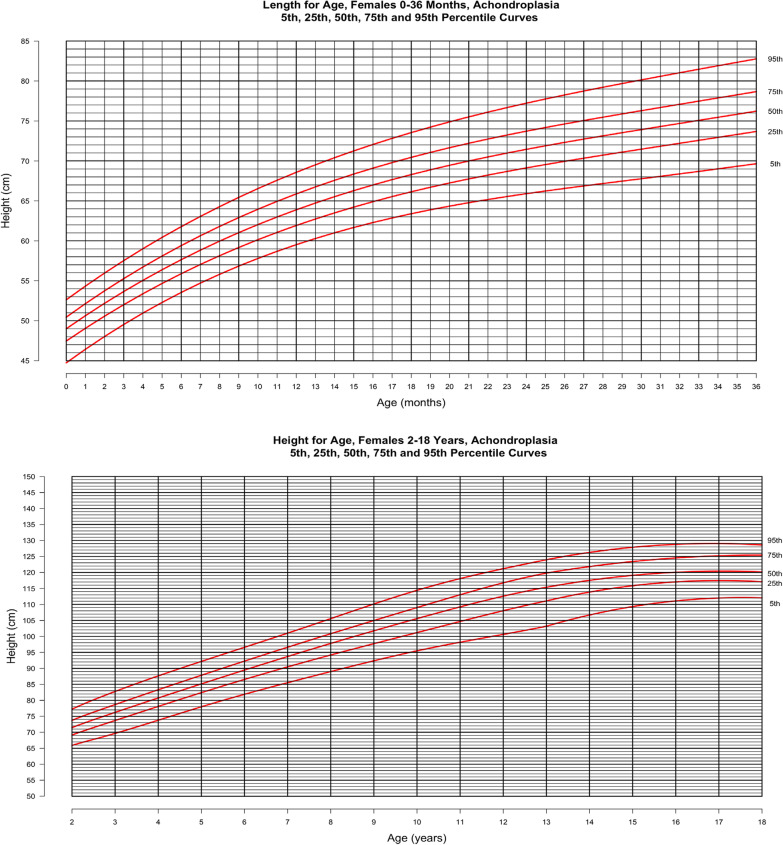
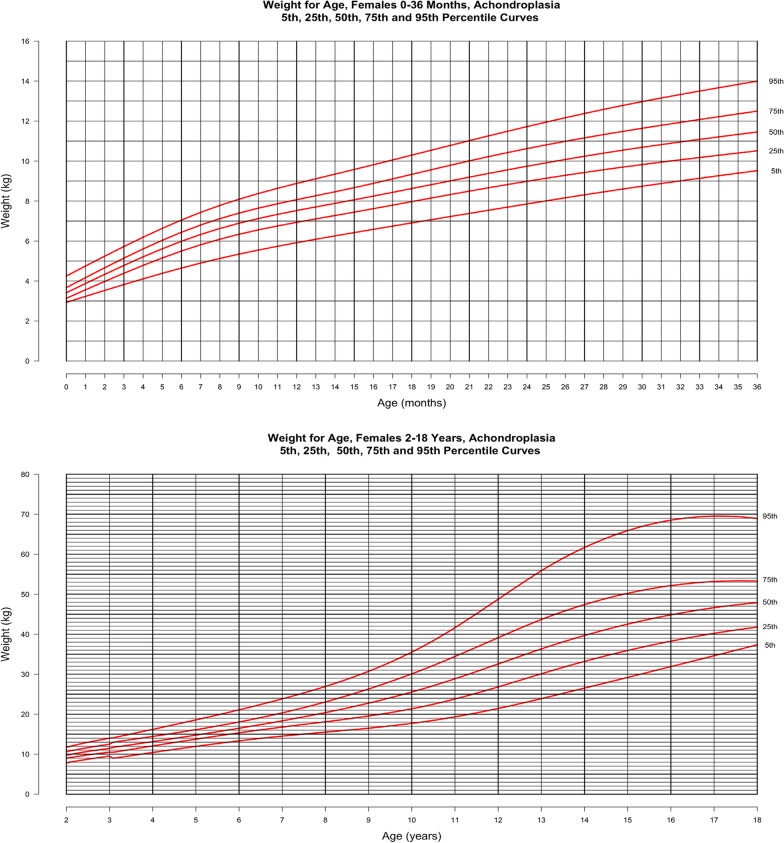
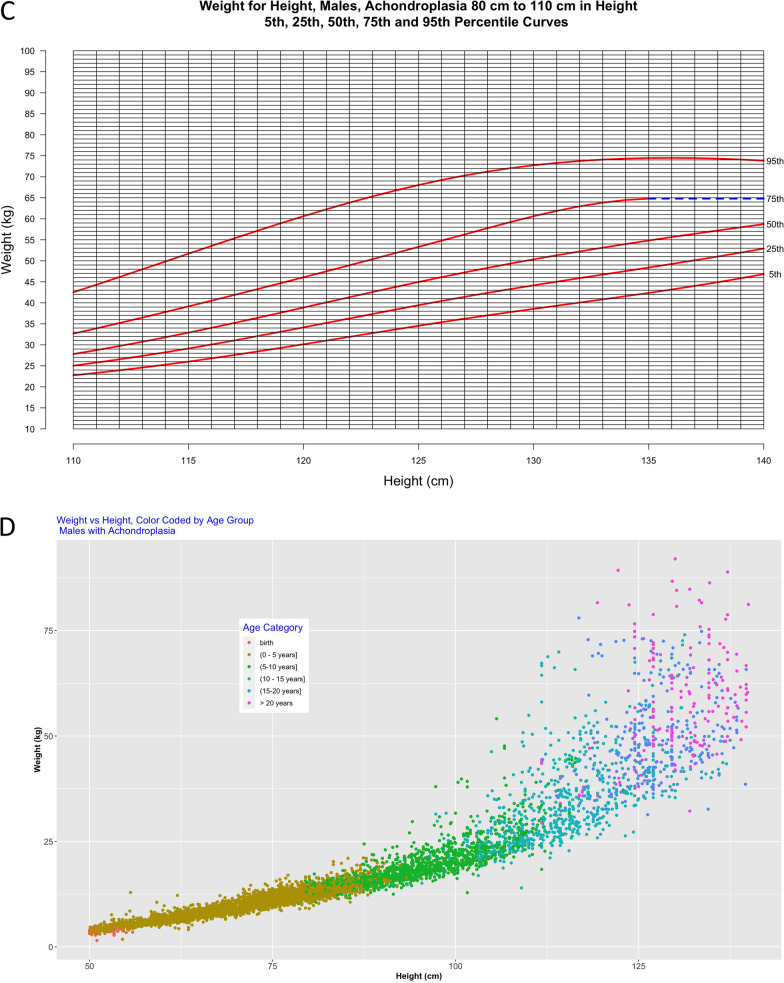
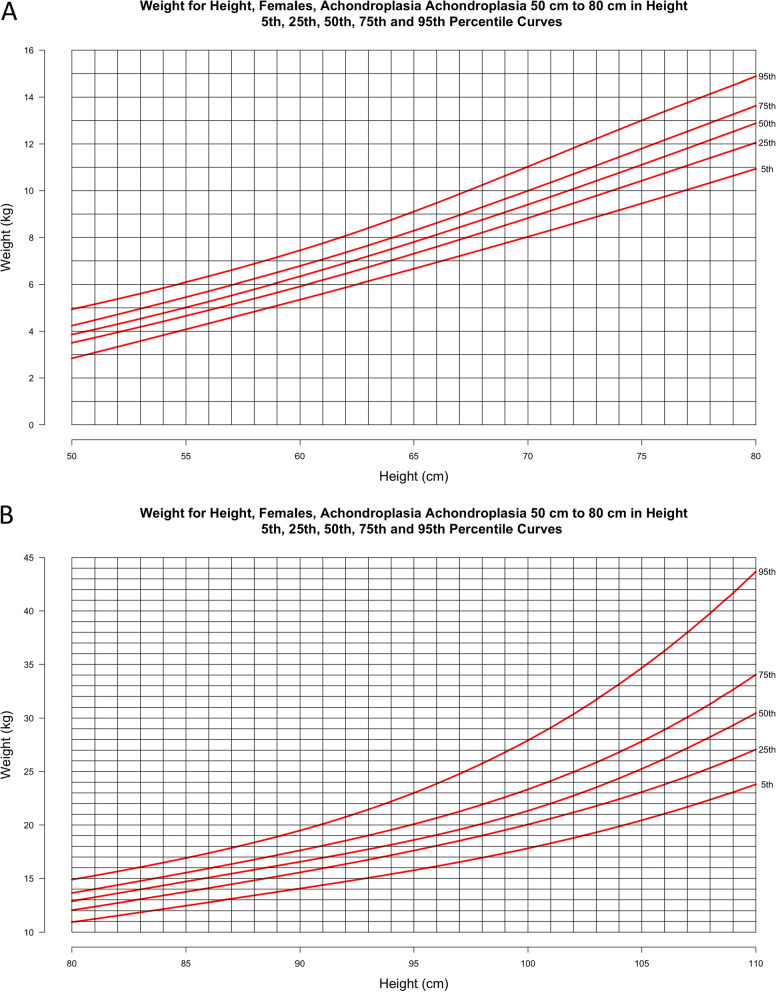
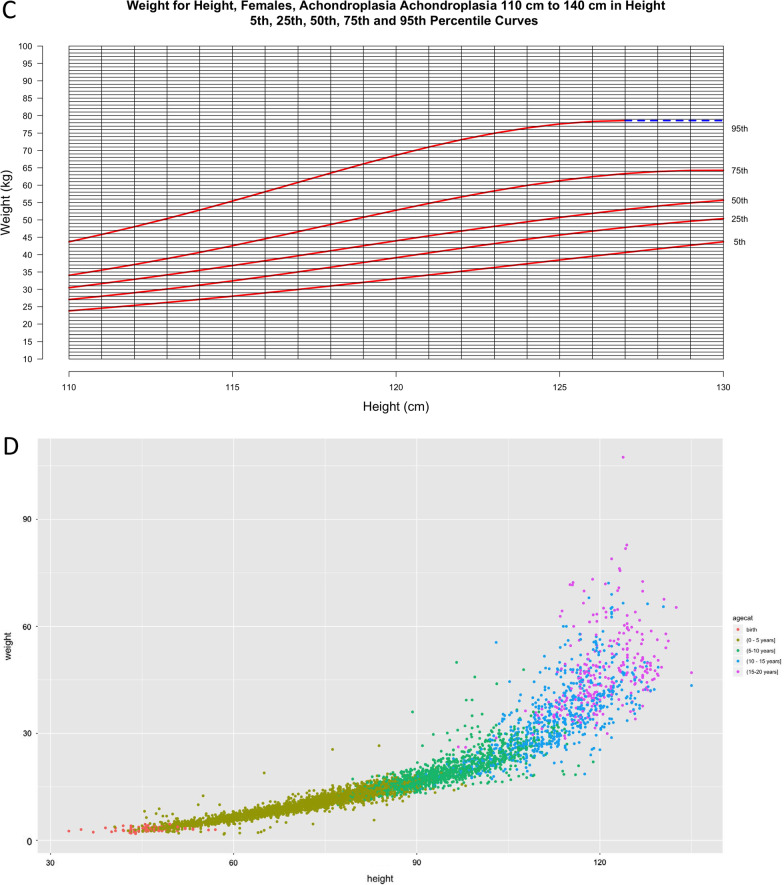
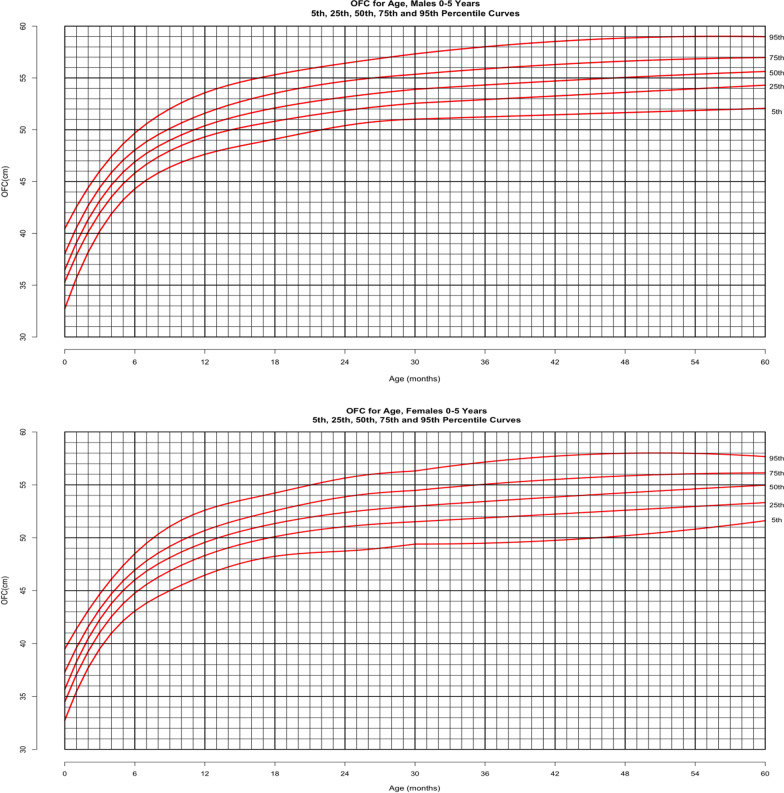
Background: Achondroplasia is the most common genetic skeletal disorder causing disproportionate short stature/dwarfism. Common additional features include spinal stenosis, midface retrusion, macrocephaly and a generalized spondylometaphyseal dysplasia which manifest as spinal cord compression, sleep disordered breathing, delayed motor skill acquisition and genu varus with musculoskeletal pain. To better understand the interactions and health outcomes of these potential complications, we embarked on a multi-center, natural history study entitled CLARITY (achondroplasia natural history study). One of the CLARITY objectives was to develop growth curves (length/height, weight, head circumference, weight-for-height) and corresponding reference tables of mean and standard deviations at 1 month increments from birth through 18 years for clinical use and research for achondroplasia patients.
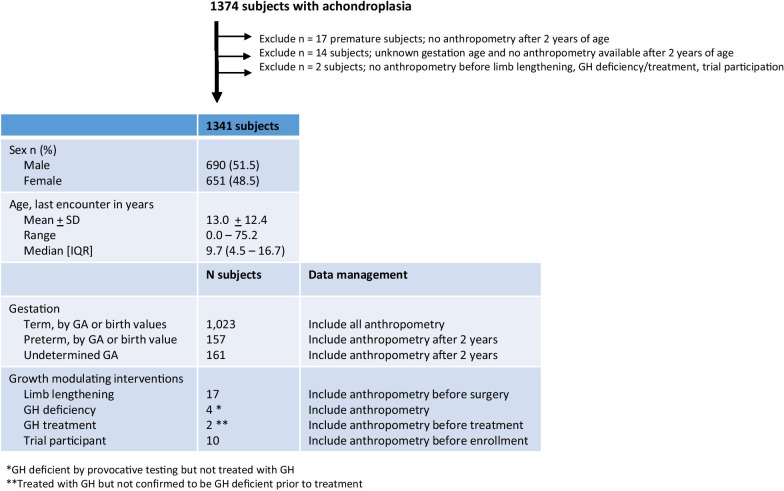
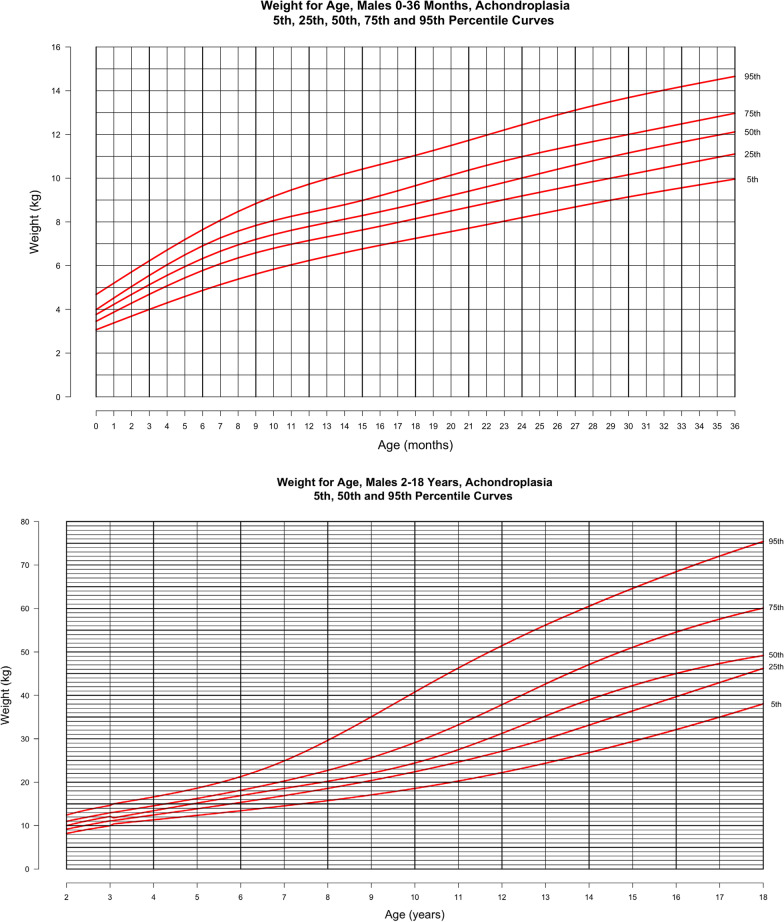
Methods: All available retrospective anthropometry data including length/height, weight and head circumference from achondroplasia patients were collected at 4 US skeletal dysplasia centers (Johns Hopkins University, AI DuPont Hospital for Children, McGovern Medical School University of Texas Health, University of Wisconsin School of Medicine and Public Health). Weight-for-age values beyond 3 SD above the mean were excluded from the weight-for-height and weight-for-age curves to create a stricter tool for weight assessment in this population.
Results: Over 37,000 length/height, weight and head circumference measures from 1374 patients with achondroplasia from birth through 75 years of age were compiled in a REDCap database. Stature and weight data from birth through 18 years of age and head circumference from birth through 5 years of age were utilized to construct new length/height-for-age, weight-for-age, head circumference-for-age and weight-for-height curves.
Conclusion: Achondroplasia-specific growth curves are essential for clinical care of growing infants and children with this condition. In an effort to provide prescriptive, rather than purely descriptive, references for weight in this population, extreme weight values were omitted from the weight-for-age and weight-for-height curves. This well-phenotyped cohort may be studied with other global achondroplasia populations (e.g. Europe, Argentina, Australia, Japan) to gain further insight into environmental or ethnic influences on growth.
Keywords: Achondroplasia; Anthropometry; Head circumference; Height/length; Weight.
© 2021. The Author(s).
Conflict of interest statement
This is an investigator-initiated independent research study supported, in part, by BioMarin, Inc. The data presented in this paper do not pertain to the investigational pharmaceuticals under development by BioMarin, Ascendis, Therachon, or QED. These following competing activities were reviewed and approved by our institutions. J.E.H.-F. has participated in Advisory Boards sponsored by BioMarin pertaining to achondroplasia. J.E.H.-F. has been consulted by BioMarin, Alexion, and Therachon/Pfizer for clinical issues related to achondroplasia and other genetic skeletal conditions and acts as a site principal investigator (PI) for clinical trials for BioMarin and Therachon/Pfizer. M.B.B. has participated in Advisory Boards sponsored by BioMarin, consulted with BioMarin, Ascendis, Therachon/Pfizer and QED for clinical issues related achondroplasia as well as acting as a site PI in their clinical trials. He is a member of Alexion’s Speaker’s Bureau (HPP). M.B.B. is a site PI and consultant for MedLife Discoveries (RCDP), and a site PI for Shire (Hunter) and SOBI (Sanfilliopo). J.T.H. has participated in Advisory Boards pertaining to achondroplasia sponsored by BioMarin. D.R.-B. has participated in Advisory Boards pertaining to achondroplasia sponsored by BioMarin. J.L. is acting as a site PI for Ascendis and has lectured for BioMarin. The other authors declare no competing interests.
Figures

References
-
- Horton WA, et al. Growth curves in achondroplasia. Birth Defects Orig Artic Ser. 1977;13(3C):101–107. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
