

Living Anatomy of the Pericardial Space: A Guide for Imaging and Interventions
- PMID: 34949433
- PMCID: PMC8712969
- DOI: 10.1016/j.jacep.2021.09.008
Living Anatomy of the Pericardial Space: A Guide for Imaging and Interventions
Abstract
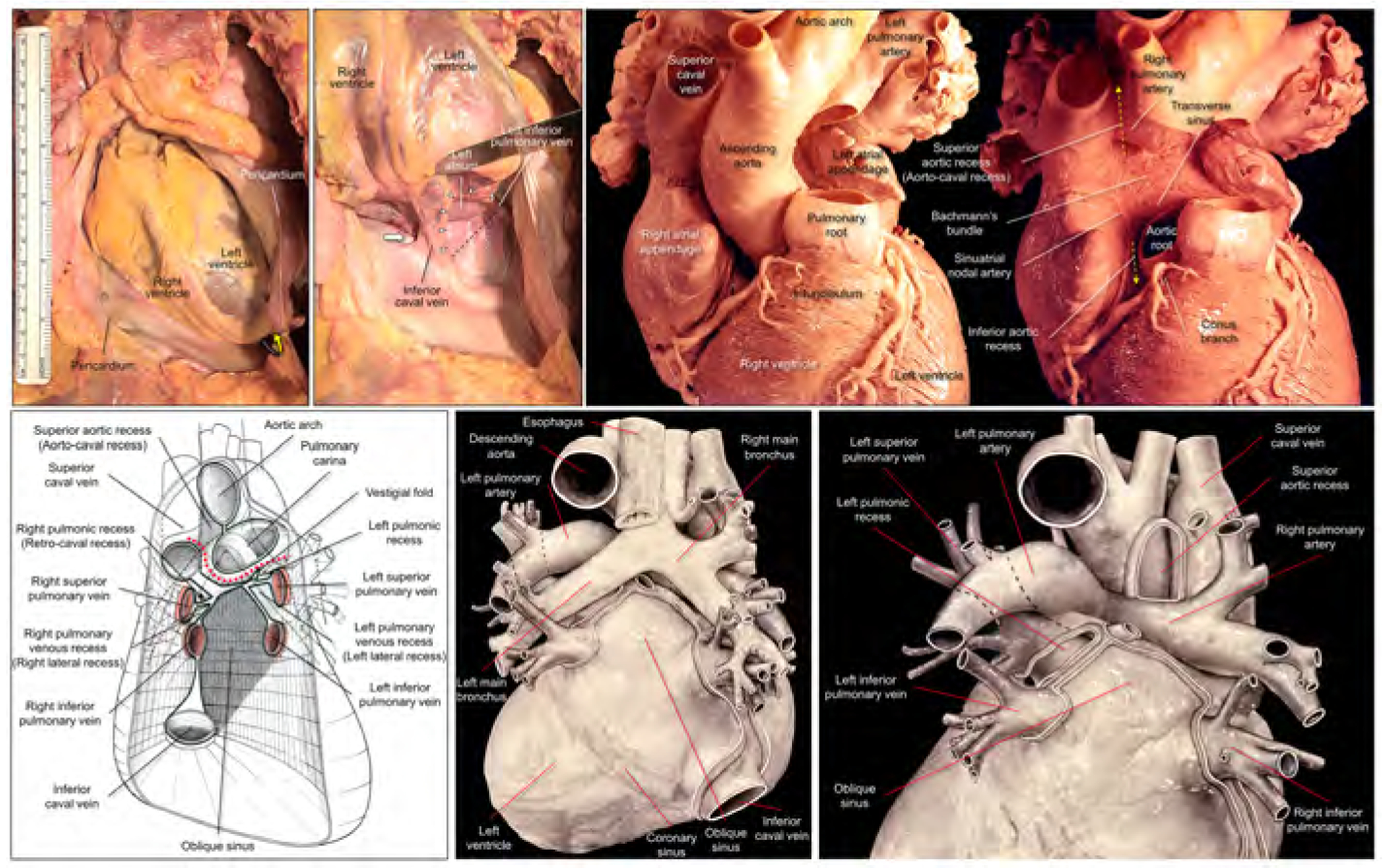
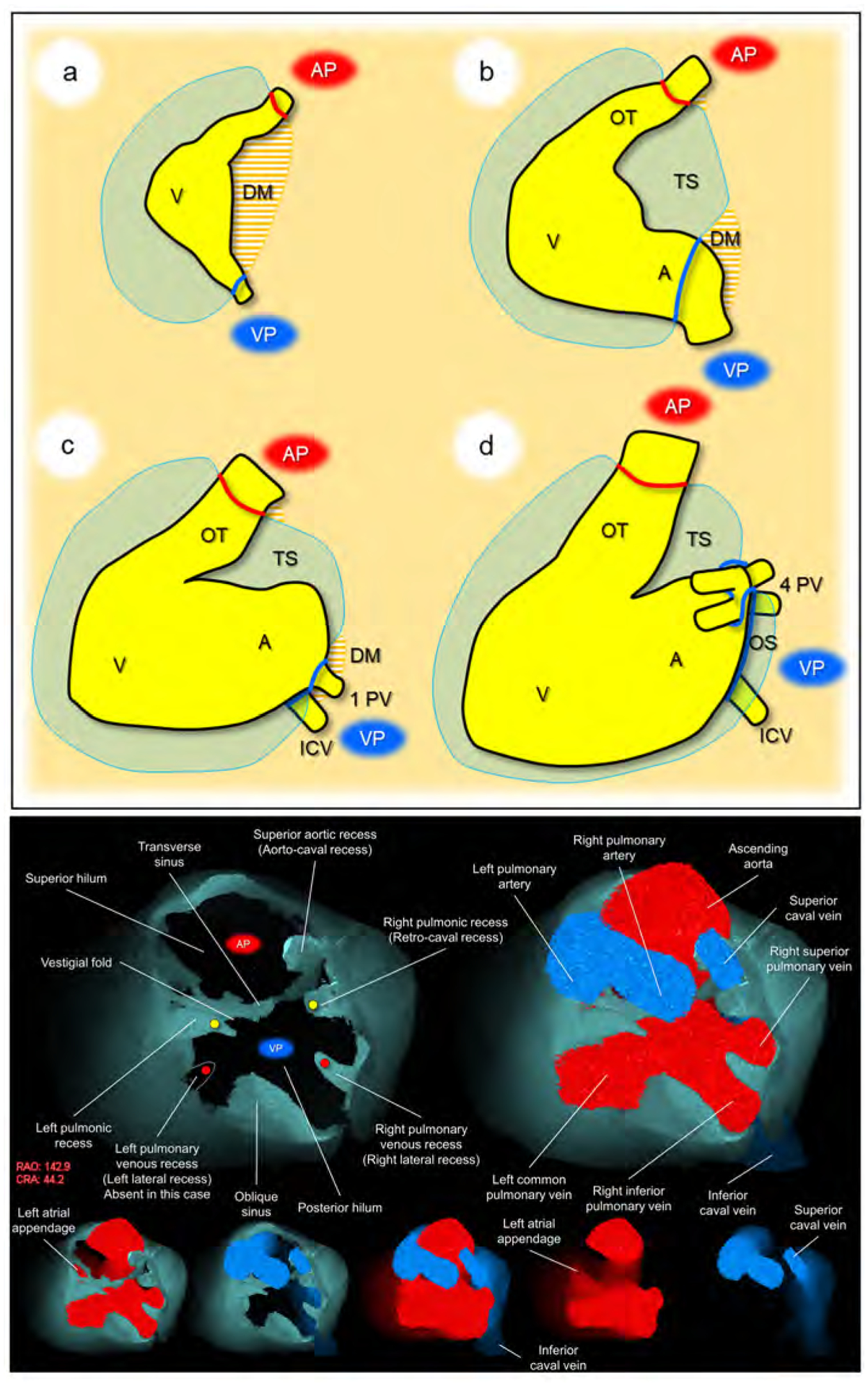
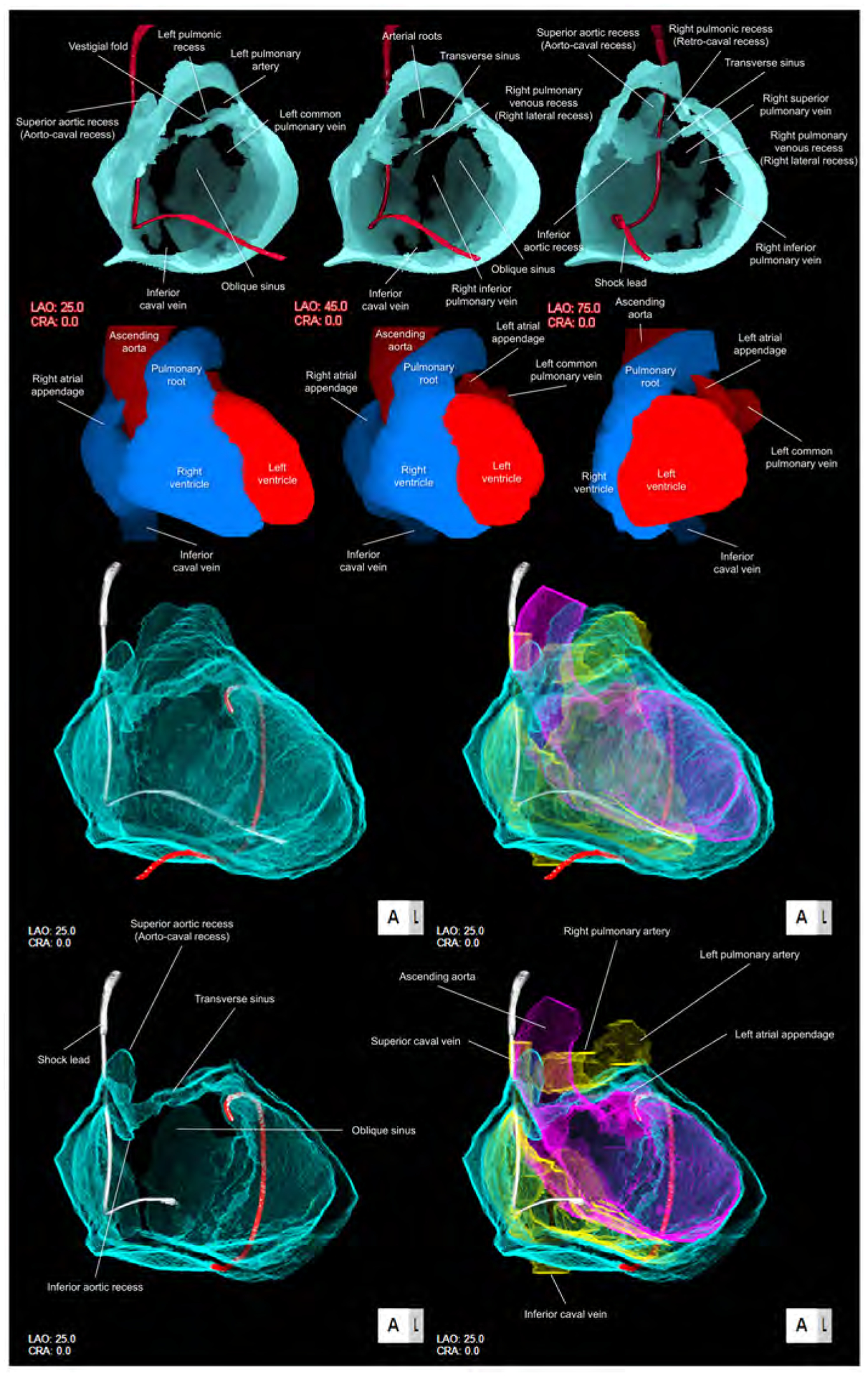
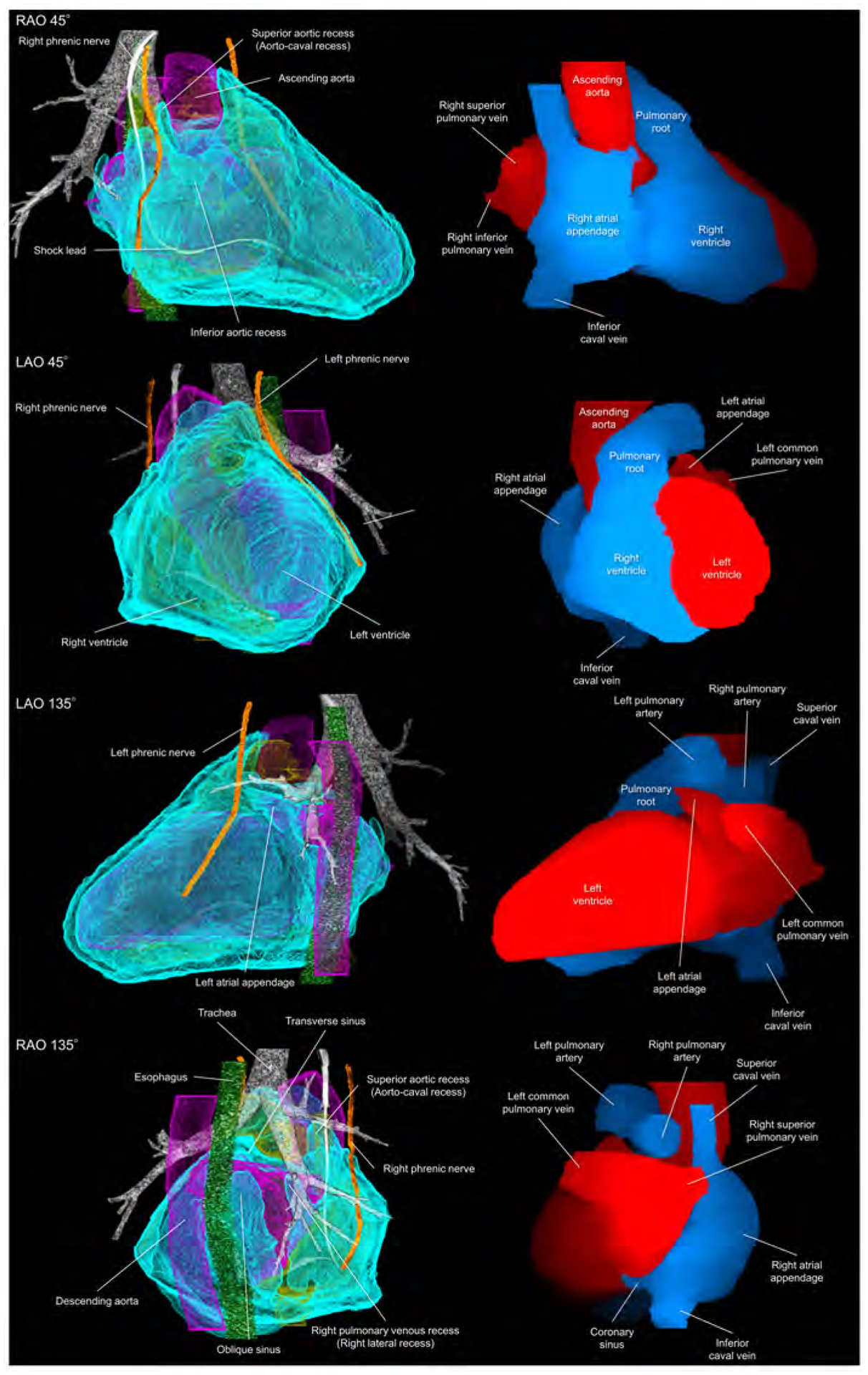
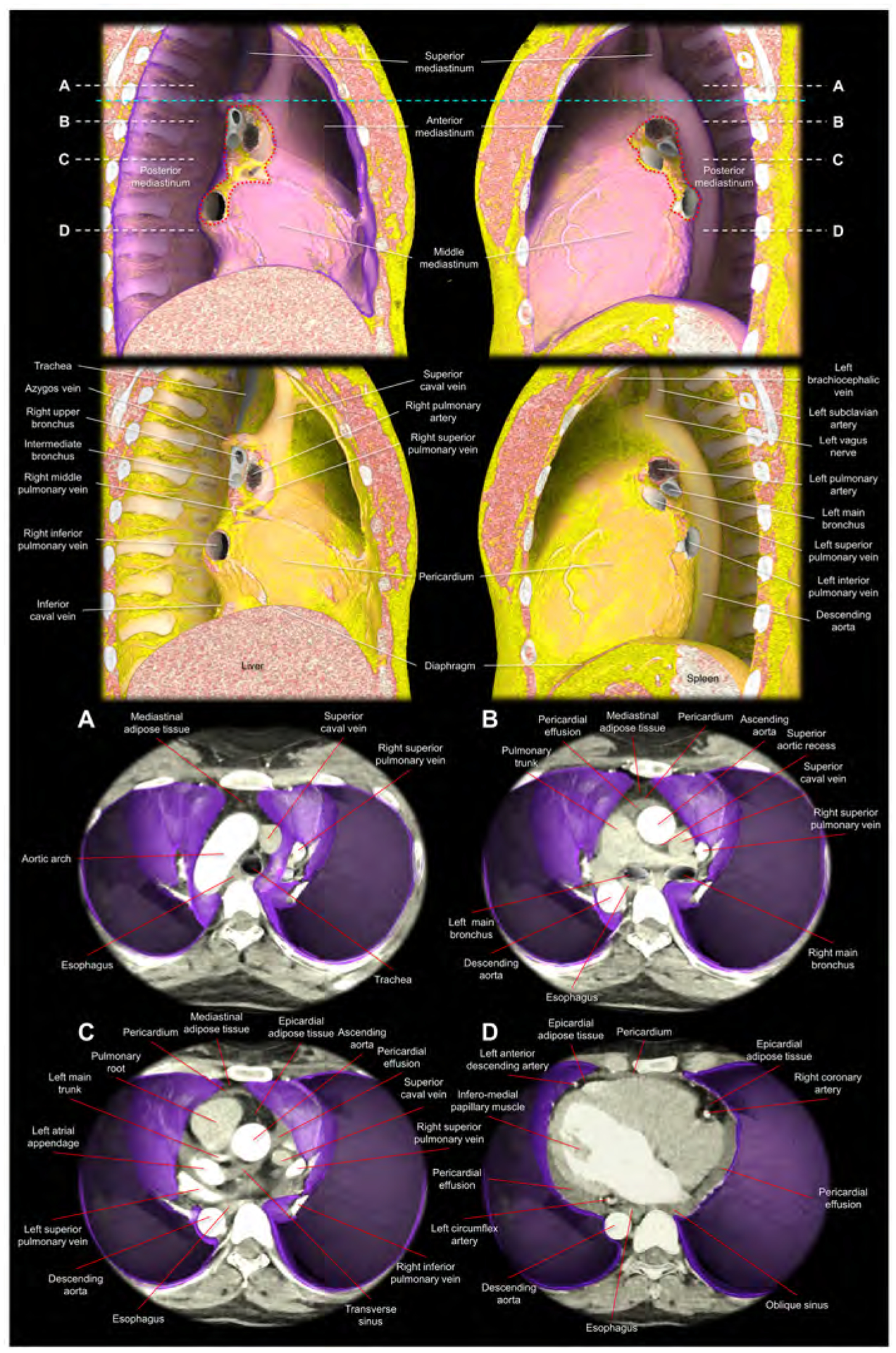
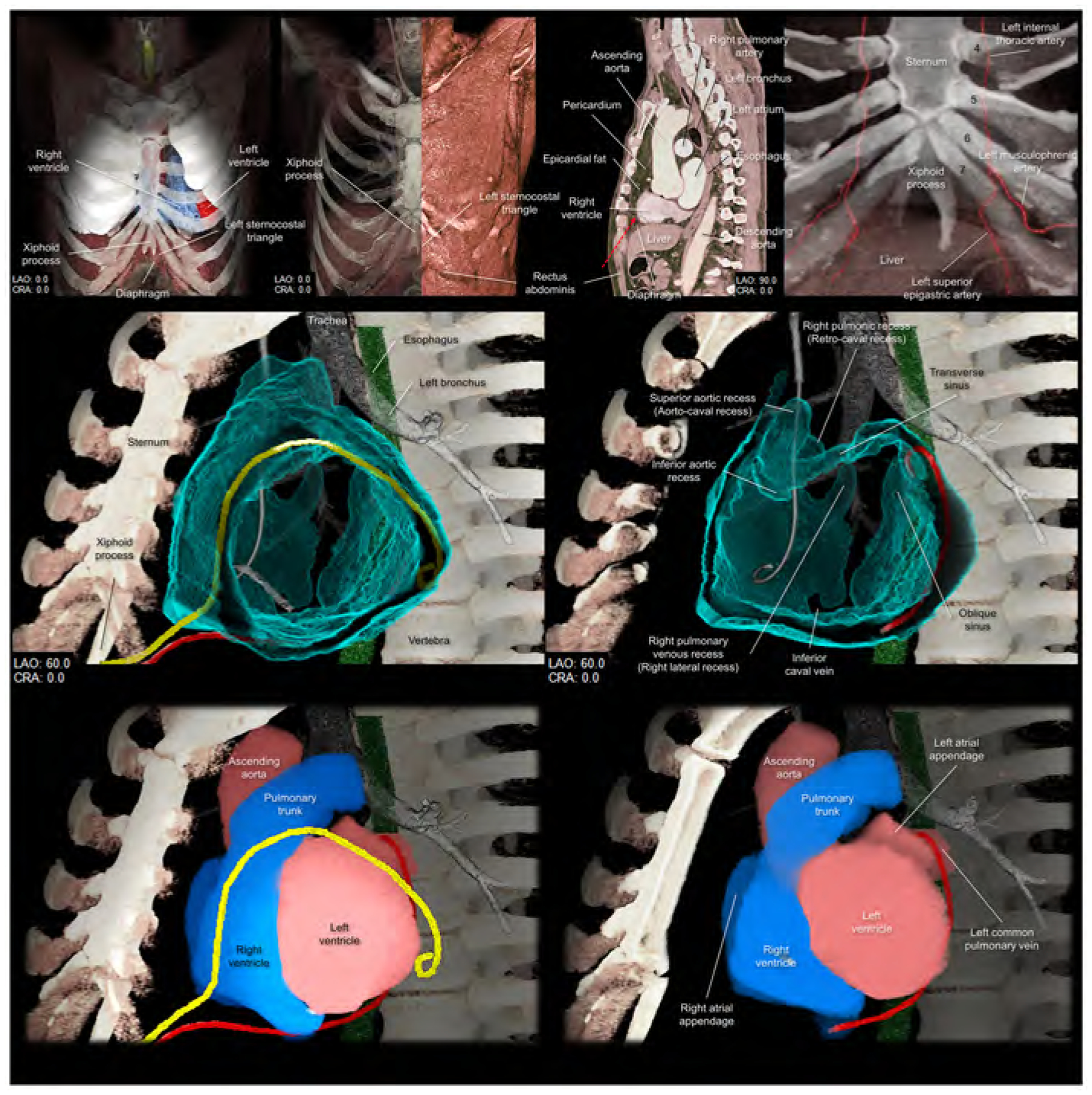
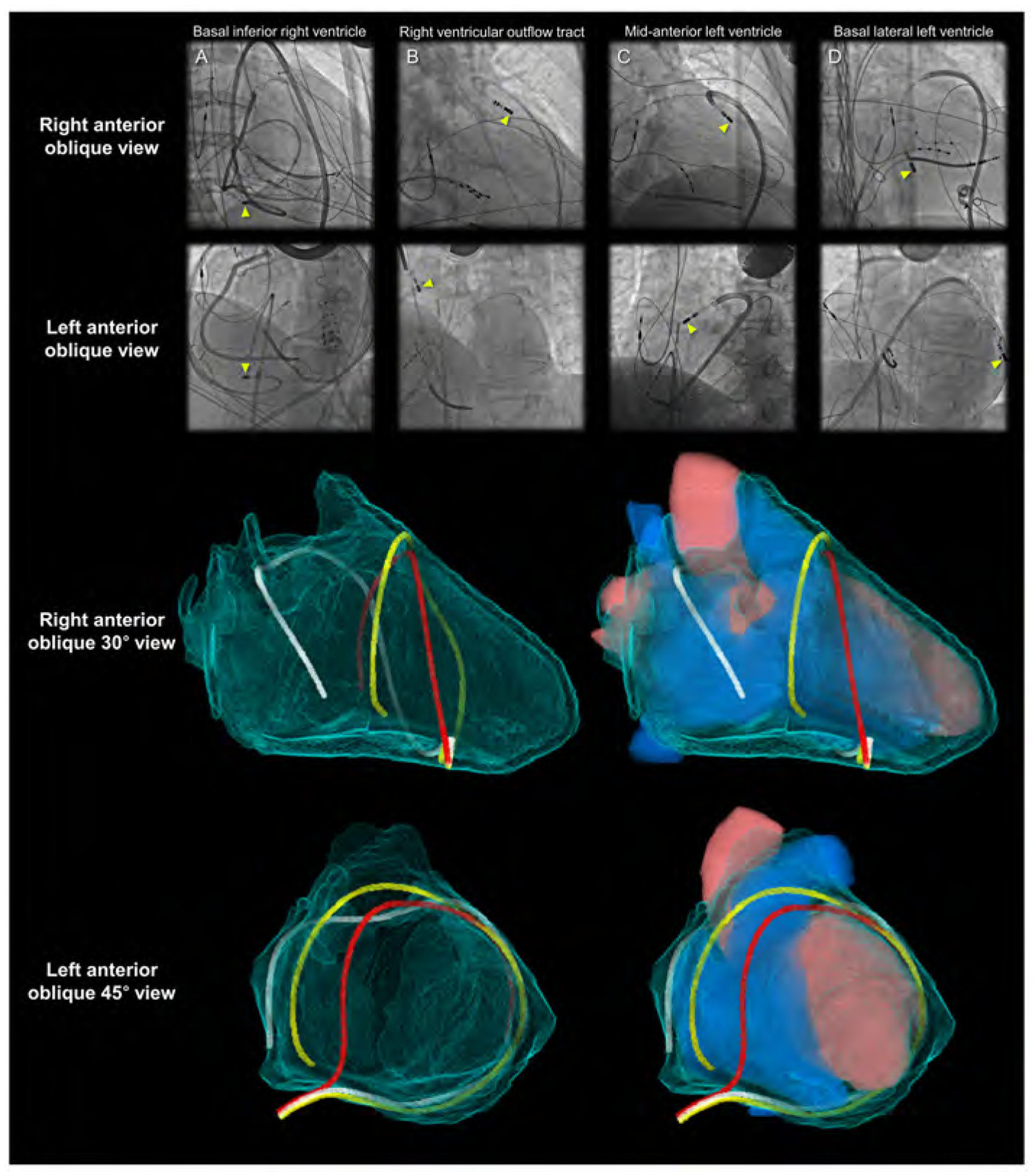
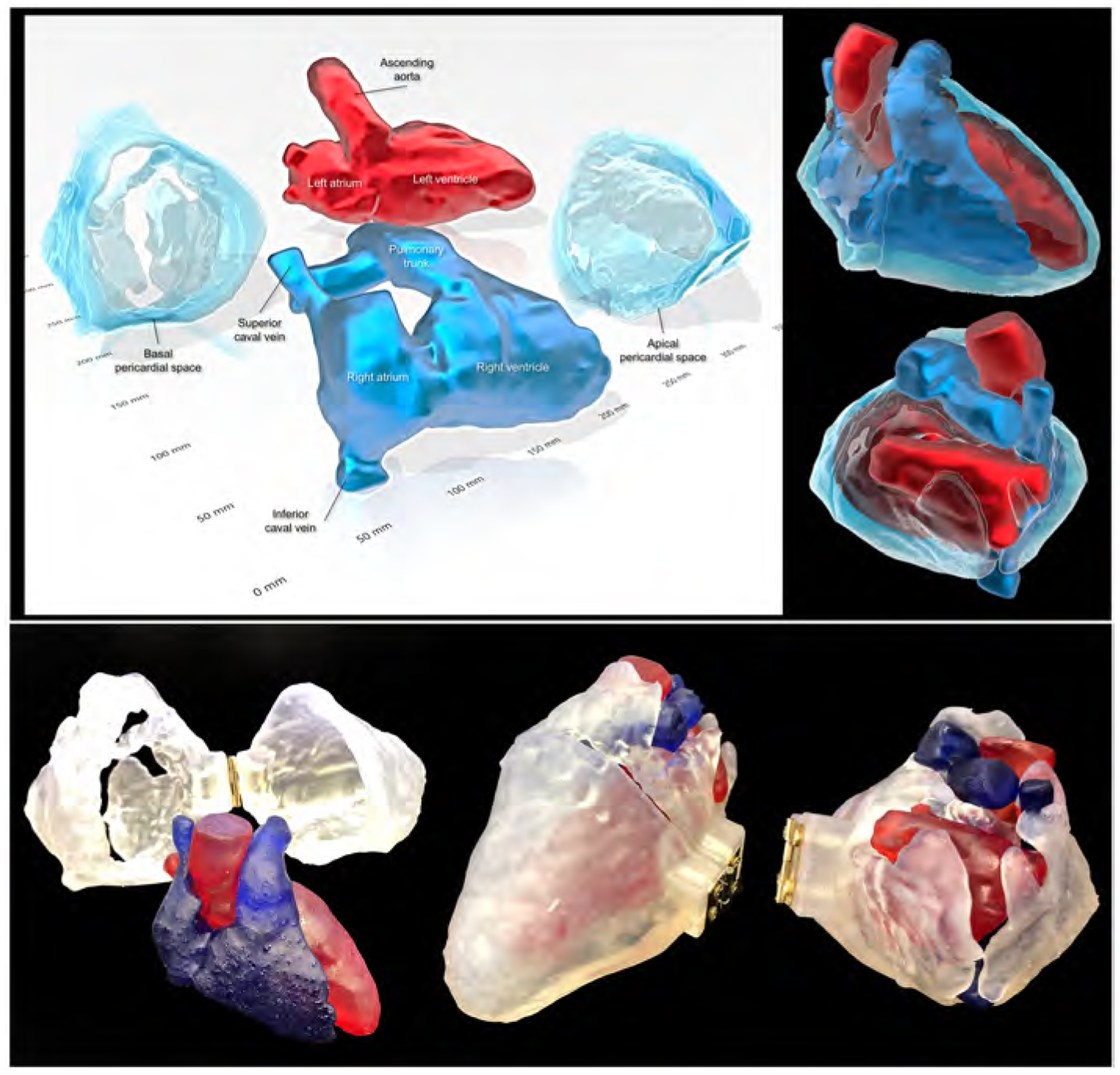
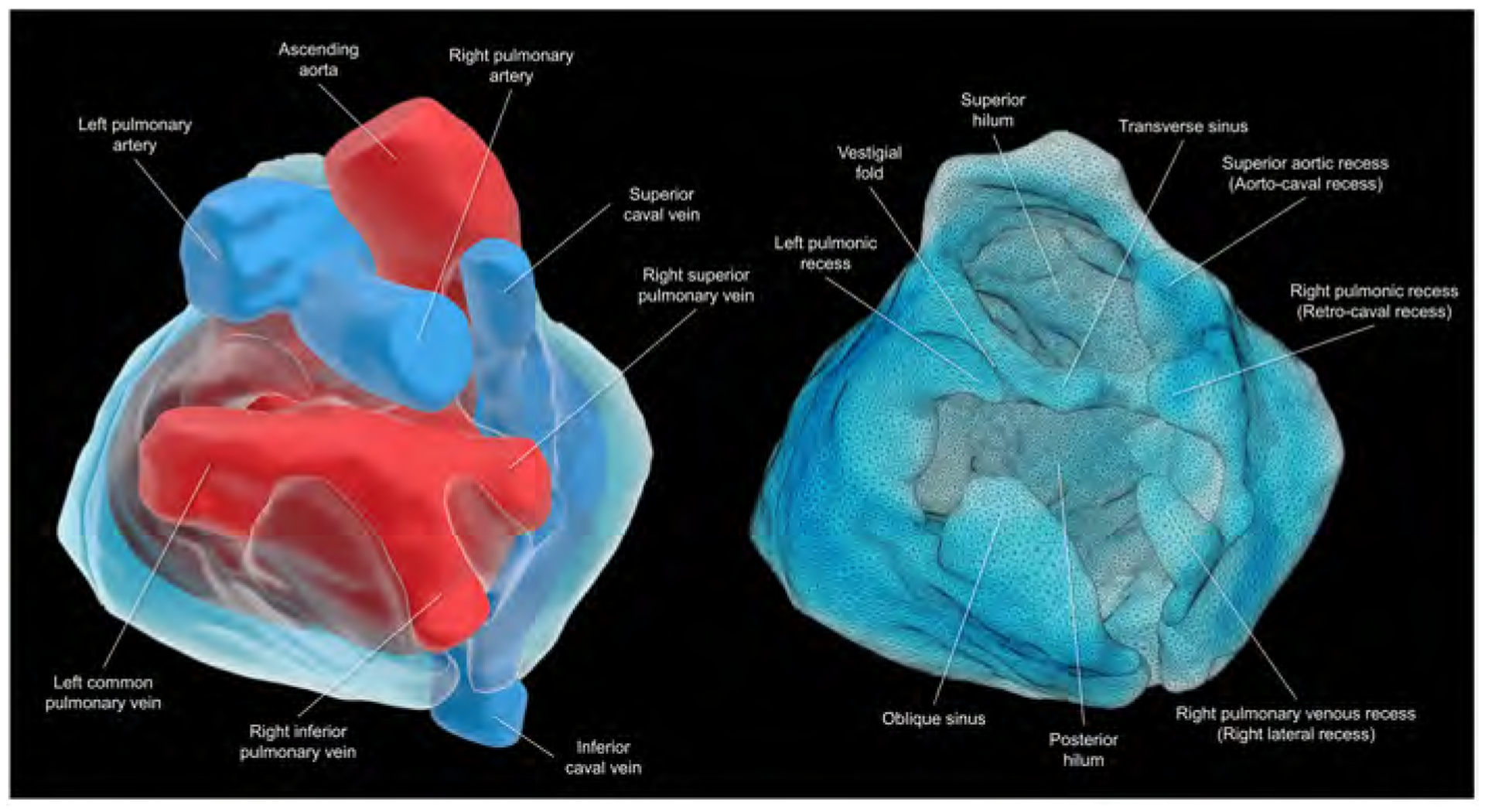
The pericardium of the human heart has received increased attention in recent times due to interest in the epicardial approach for cardiac interventions to treat cardiac arrhythmias refractory to conventional endocardial approaches. To support further clinical application of this technique, it is fundamental to appreciate the living anatomy of the pericardial space, as well as its relationships to the surrounding structures. The anatomy of the pericardial space, however, is extremely difficult regions to visualize. This is due to its complex 3-dimensionality, and the "potential" nature of the space, which becomes obvious only when there is collection of pericardial fluid. This potential space, which is bounded by the epicardium and pericardium, can now be visualized by special techniques as we now report, permitting appreciation of its living morphology. Current sources of knowledge are limited to the dissection images, surgical images, and/or illustrations, which are not necessarily precise or sufficient to provide relevant comprehensive anatomical knowledge to those undertaking the epicardial approach. The authors demonstrate, for the first time to their knowledge, the 3-dimensional living anatomy of the pericardial space relative to its surrounding structures. They also provide correlative anatomy of the left sternocostal triangle as a common site for subxiphoid access. The authors anticipate their report serving as a tool for education of imaging and interventional specialists.
Keywords: cardiac anatomy; computed tomography; pericardial recess; pericardial sinus; pericardial space.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was made possible by support from National Institutes of Health grant OT2OD023848 to Dr Shivkumar. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Sosa E, Scanavacca M, d’Avila A, Pilleggi F. A new technique to perform epicardial mapping in the electrophysiology laboratory. J Cardiovasc Electrophysiol 1996;7:531–6. - PubMed
-
- Wood MA. Percutaneous pericardial instrumentation in the electrophysiology laboratory: a case of need. Heart Rhythm 2006;3:11–2. - PubMed
-
- Sacher F, Roberts-Thomson K, Maury P, et al. Epicardial ventricular tachycardia ablation a multicenter safety study. J Am Coll Cardiol 2010;55:2366–72. - PubMed
-
- Swale M, Mikell S, Gard J, Munger TM, Asirvatham SJ, Friedman PA. Epicardial access: patient selection, anatomy, and a stepwise approach. J Innov Card Rhythm Manag 2011;2:239–49.
