A New Implantable Closed-Loop Clinical Neural Interface: First Application in Parkinson's Disease
- PMID: 34949982
- PMCID: PMC8689059
- DOI: 10.3389/fnins.2021.763235
A New Implantable Closed-Loop Clinical Neural Interface: First Application in Parkinson's Disease
Abstract
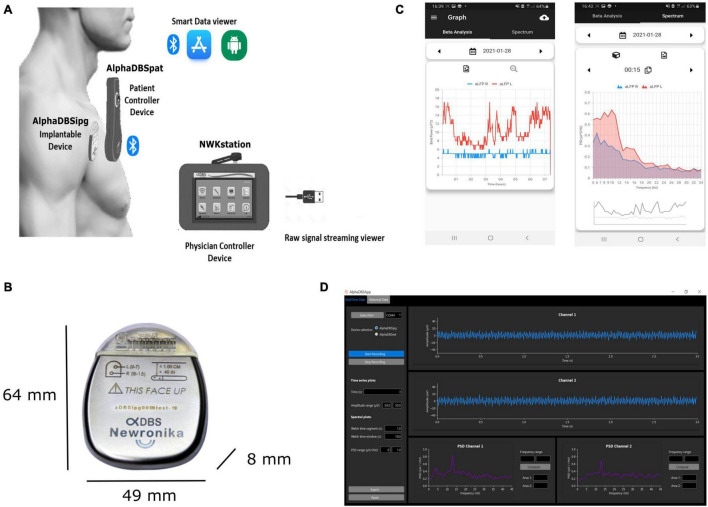
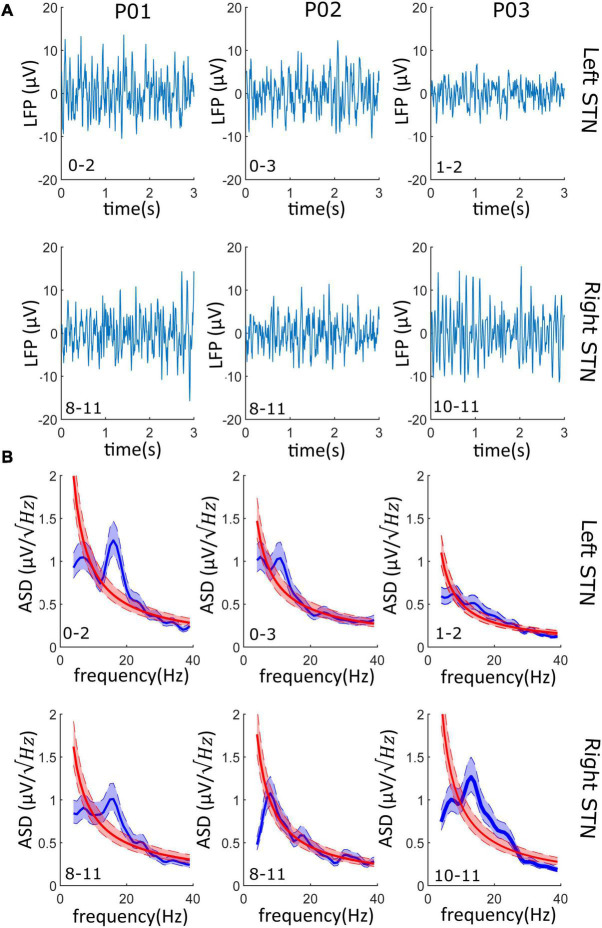
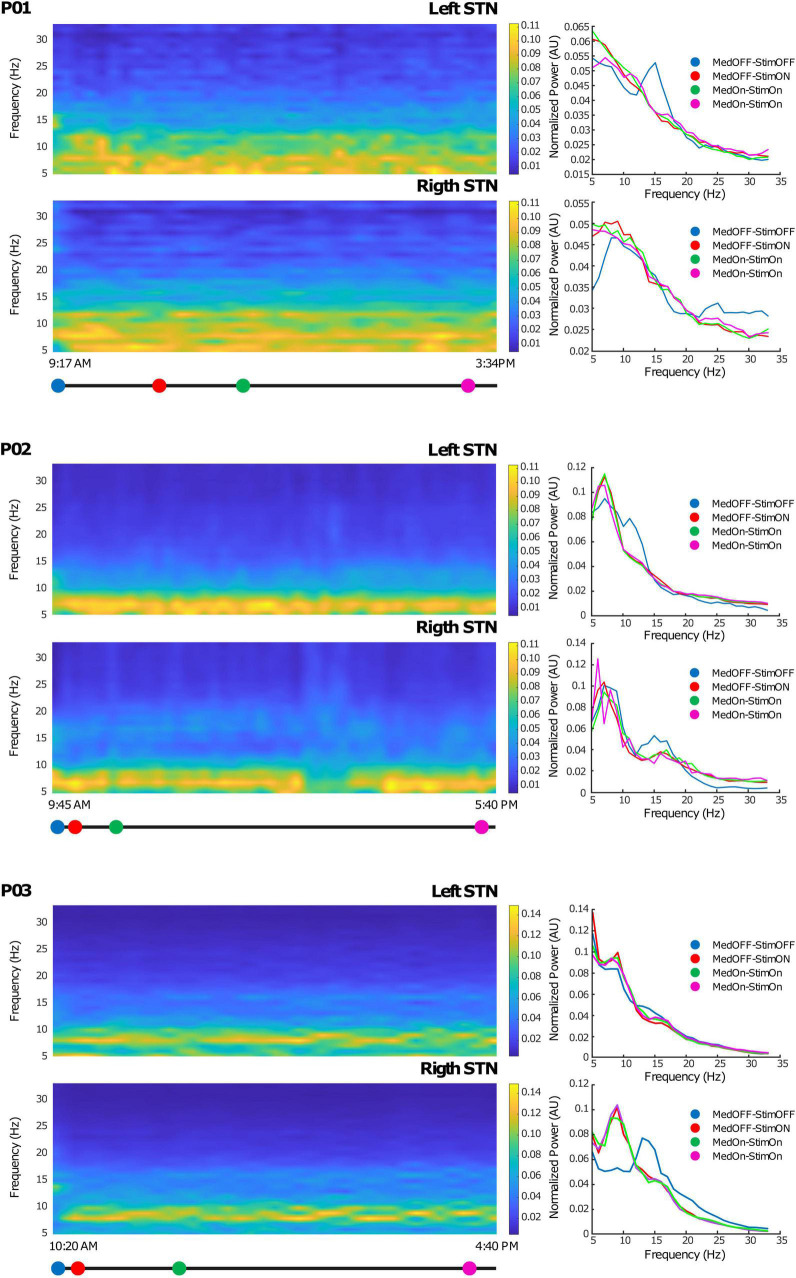
Deep brain stimulation (DBS) is used for the treatment of movement disorders, including Parkinson's disease, dystonia, and essential tremor, and has shown clinical benefits in other brain disorders. A natural path for the improvement of this technique is to continuously observe the stimulation effects on patient symptoms and neurophysiological markers. This requires the evolution of conventional deep brain stimulators to bidirectional interfaces, able to record, process, store, and wirelessly communicate neural signals in a robust and reliable fashion. Here, we present the architecture, design, and first use of an implantable stimulation and sensing interface (AlphaDBSR System) characterized by artifact-free recording and distributed data management protocols. Its application in three patients with Parkinson's disease (clinical trial n. NCT04681534) is shown as a proof of functioning of a clinically viable implanted brain-computer interface (BCI) for adaptive DBS. Reliable artifact free-recordings, and chronic long-term data and neural signal management are in place.
Keywords: Parkinson’s disease; closed-loop; deep brain stimulation; implantable device; local field potential (LFP); neural interface; neuromodulation.
Copyright © 2021 Arlotti, Colombo, Bonfanti, Mandat, Lanotte, Pirola, Borellini, Rampini, Eleopra, Rinaldo, Romito, Janssen, Priori and Marceglia.
Conflict of interest statement
MA and MC were employed by Newronika and held stock options. AB is a consultant for Newronika. AP, SM, and PR are founders and shareholders of Newronika. The study was funded by Newronika SpA. The funder had the following involvement with the study: study design of NCT04681534, signal collection and analysis (clinical data collection is performed by a CRO), the writing of this article, and the decision to submit it for publication. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures