

Advanced lipoprotein parameters could better explain atheromatosis in non-diabetic chronic kidney disease patients
- PMID: 34950470
- PMCID: PMC8690051
- DOI: 10.1093/ckj/sfab113
Advanced lipoprotein parameters could better explain atheromatosis in non-diabetic chronic kidney disease patients
Abstract
Background: Chronic kidney disease (CKD) patients have a high burden of atheromatous cardiovascular disease (ASCVD) not fully explained by traditional lipid parameters. Lipoprotein composition and subclass particle number information could improve ASCVD risk assessment. The objective of this study is to investigate the association of advanced lipoprotein parameters with the risk of atheromatosis in a subpopulation of the NEFRONA study.
Methods: This was a cross-sectional study in 395 non-diabetic individuals (209 CKD and 186 non-diabetic and non-CKD) without statin therapy. Vascular ultrasound examination assessing 10 territories was combined with advanced lipoprotein testing performed by nuclear magnetic resonance spectroscopy. Logistic regression was used to estimate adjusted odds ratios (ORs) per 1 standard deviation increment.
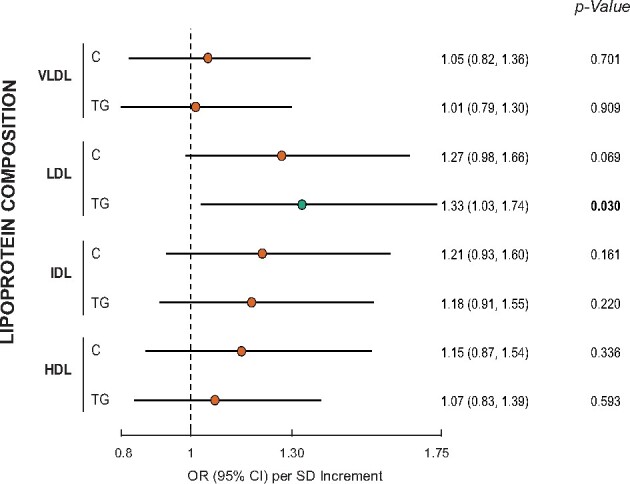
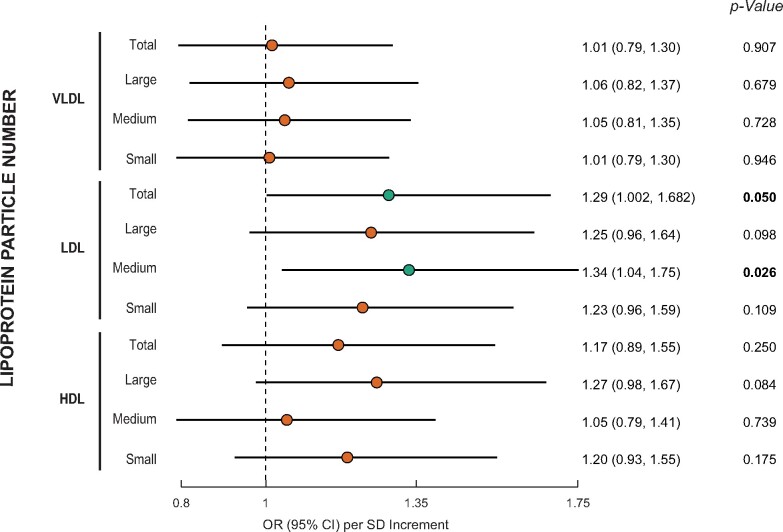
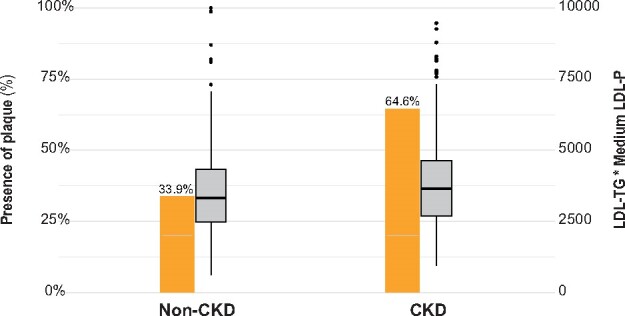
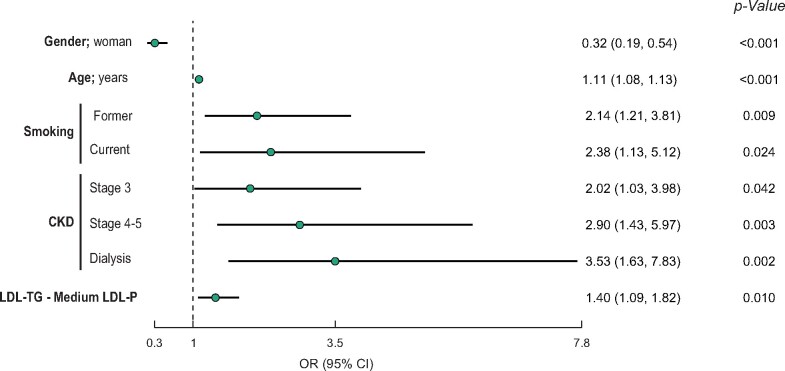
Results: Atheromatosis was more prevalent in CKD patients (33.9% versus 64.6%). After adjusting for age, gender, smoking habit and CKD stage, the amount of triglycerides (TGs) within low-density lipoprotein (LDL) lipoproteins was independently and positively associated with atheromatosis [OR 1.33; 95% confidence interval (CI) 1.03-1.74; P = 0.03]. Similarly, total and medium LDL particles (LDL-Ps) showed a positive association (OR 1.29; 95% CI 1.00-1.68; P = 0.05 and OR 1.34; 95% CI 1.04-1.75; P = 0.03, respectively). TG-loaded medium LDL-Ps were higher in CKD patients compared with controls and showed an adjusted OR of 1.40 (95% CI 1.09-1.82; P = 0.01) in non-diabetic patients (CKD and non-CKD individuals). In contrast, non-diabetic CKD patients showed a similar coefficient but the significance was lost (OR 1.2; 95% CI 0.8-1.7; P = 0.359).
Conclusions: Non-diabetic CKD patients showed a higher amount of TG-loaded medium LDL-Ps compared with controls. These particles were independently associated with atheromatosis in non-diabetic patients.
Keywords: LDL cholesterol; atherosclerosis; chronic kidney disease; dyslipidemia; lipoprotein subfractions; triglycerides.
© The Author(s) 2021. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
Similar articles
-
An in-depth analysis shows a hidden atherogenic lipoprotein profile in non-diabetic chronic kidney disease patients.Expert Opin Ther Targets. 2019 Jul;23(7):619-630. doi: 10.1080/14728222.2019.1620206. Epub 2019 May 23. Expert Opin Ther Targets. 2019. PMID: 31100024
-
Prevalence of subclinical atheromatosis and associated risk factors in chronic kidney disease: the NEFRONA study.Nephrol Dial Transplant. 2014 Jul;29(7):1415-22. doi: 10.1093/ndt/gfu038. Epub 2014 Feb 28. Nephrol Dial Transplant. 2014. PMID: 24586070
-
Observational multicenter study to evaluate the prevalence and prognosis of subclinical atheromatosis in a Spanish chronic kidney disease cohort: baseline data from the NEFRONA study.BMC Nephrol. 2014 Oct 18;15:168. doi: 10.1186/1471-2369-15-168. BMC Nephrol. 2014. PMID: 25326683 Free PMC article.
-
Lowering Targeted Atherogenic Lipoprotein Cholesterol Goals for Patients at "Extreme" ASCVD Risk.Curr Diab Rep. 2019 Nov 21;19(12):146. doi: 10.1007/s11892-019-1246-y. Curr Diab Rep. 2019. PMID: 31754844 Review.
-
2017 Taiwan lipid guidelines for high risk patients.J Formos Med Assoc. 2017 Apr;116(4):217-248. doi: 10.1016/j.jfma.2016.11.013. Epub 2017 Feb 24. J Formos Med Assoc. 2017. PMID: 28242176 Review.
Cited by
-
Therapeutic effect and potential mechanism of Fufang Danshen dripping pills for stable coronary heart disease: a randomized controlled trial.Front Cardiovasc Med. 2025 Jan 29;12:1506917. doi: 10.3389/fcvm.2025.1506917. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 39944604 Free PMC article.
-
Use of lipid-lowering therapies in patients with chronic kidney disease and atherosclerotic cardiovascular disease: 2-year results from Getting to an imprOved Understanding of Low-Density lipoprotein cholesterol and dyslipidemia management (GOULD).Clin Cardiol. 2022 Dec;45(12):1303-1310. doi: 10.1002/clc.23923. Epub 2022 Sep 19. Clin Cardiol. 2022. PMID: 36124341 Free PMC article.
-
Lipid Profile and Cardiovascular Risk Modification after Hepatitis C Virus Eradication.Pathogens. 2024 Mar 25;13(4):278. doi: 10.3390/pathogens13040278. Pathogens. 2024. PMID: 38668233 Free PMC article. Review.
References
-
- Benjamin EJ, Virani SS, Callaway CW et al.; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2018 update: A report from the American Heart Association. Circulation 2018; 137: e67–e492 - PubMed
-
- Boekholdt SM, Arsenault BJ, Mora S et al. Association of LDL cholesterol, non-HDL cholesterol, and apolipoprotein B levels with risk of cardiovascular events among patients treated with statins: a meta-analysis. JAMA 2012; 307: 1302–1309 - PubMed
-
- Ference BA, Ginsberg HN, Graham I et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J 2017; 38: 2459–2472 - PMC - PubMed
-
- Musliner TA, Krauss RM. Lipoprotein subspecies and risk of coronary disease. Clin Chem 1988; 34: B78–B83 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
